J Res Health Sci. 21(1):e00503.
doi: 10.34172/jrhs.2021.39
Review Article
Kidney Complications of COVID-19: A Systematic Review and Meta-Analysis
Naser Nasiri 1, Shoboo Rahmati 1, Abbas Etminan 2, Hamid Sharifi 3, Azam Bazrafshan 3, Mohammad Karamouzian 3, 4, Ali Sharifi 5, *
Author information:
1Student Research Committee, Kerman University of Medical Sciences, Kerman, Iran
2Department of Internal Medicine, School of Medicine, Endocrinology and Metabolism Research Center, Afzalipour Hospital, Kerman University of Medical Sciences, Kerman, Iran
3HIV/STI Surveillance Research Center, and WHO Collaborating Center for HIV Surveillance, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
4School of Population and Public Health, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
5Department of Ophthalmology, Shafa Hospital, Afzalipour School of Medicine, Kerman University of Medical Sciences, Kerman, Iran
Abstract
Background: Some patients with coronavirus disease 2019 (COVID-19) have been reported to have developed mild to severe kidney injuries. The current systematic review and meta-analysis was carried out to estimate the prevalence and incidence of acute kidney injury (AKI) among COVID-19 patients.
Study design: A systematic review and meta-analysis
Methods: PubMed, Embase, Scopus, Web of Science, and MedRxiv databases were searched from December 1, 2019, up to July 27, 2020. Two independent co-authors completed the screening process, data extraction, and quality assessment of the retrieved records. Random-effects meta-analyses were used to determine the pooled prevalence and 95% confidence interval (CI) of AKI among COVID-19 patients.
Results: Out of 2,332 unique identified records, 51 studies were included in the review. Overall, the studies were carried out on 25,600 patients. A total of 6,505 patients (in 18 cross-sectional studies) were included to estimate the pooled prevalence of AKI, and 18,934 patients (in 27 cohort studies) were included to determine the pooled incidence of AKI. The pooled prevalence of AKI was estimated as 10.08% (95% CI: 4.59, 17.32; I 2=98.56%; P<0.001). Furthermore, the pooled incidence of AKI was 12.78% (95% CI: 7.38, 19.36; I 2=99.27%; P<0.001). The mean (95% CI) values of serum creatinine (SCr), blood urea nitrogen (BUN), potassium, and sodium were 76.10 (69.36, 82.84), 4.60 (4.04, 5.30), 3.94 (3.78, 4.11), and 139.30 (138.26, 140.36) mmol/L, respectively.
Conclusions: The AKI is a considerable complication among COVID-19 patients and should be screened for on clinical examinations. The BUN, SCr, potassium, and sodium levels were within the normal ranges.
Keywords: Prevalence, Acute kidney injury, COVID-19, Blood urea nitrogen, Creatinine
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Citation: Nasiri N, Rahmati S, Etminan A, Sharifi H, Bazrafshan A, Karamouzian A, Sharifi A. Kidney Complications of COVID-19: A Systematic Review and Meta-Analysis. J Res Health Sci. 2021; 21(1): e00503.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) rapidly spread around the globe
1
, and coronavirus disease 2019 (COVID-19) was declared a pandemic by the World Health Organization in March 2020
2
. By October 11, 2020, more than 37 million individuals had been infected with COVID-19, and 1,078,715 cases had died due to COVID-19
3
. The SARS-CoV-2 enters the host cells and binds to angiotensin-converting enzyme 2 (ACE2) receptors
1
. Most COVID-19 patients have multiple signs or symptoms; however, commonly reported signs and symptoms are fever, fatigue, dry cough, and muscular pain
4
. COVID-19 is more common among individuals with multimorbidities, such as hypertension, diabetes, cardiovascular, and respiratory diseases
5
.
Different internal organs, such as heart, liver, and kidney, can be damaged in COVID-19 patients
6
. The results of studies showed that ACE2 is the central receptor to enter pathogens in human cells
7,8
. The ACE2 is expressed in kidneys
9
and exists in proximal tubule cells
8
. The SARS-CoV-2 can particularly affect kidneys and lead to acute kidney injury (AKI)
9
. Several studies have reported AKI and increased blood urea nitrogen (BUN) and serum creatinine (SCr) in COVID-19 patients
6,10,11
. For example, Yang et al. reported that 13.7% and 9.6% of COVID-19 patients had elevated BUN and SCr levels, respectively
10
. Moreover, AKI has also been shown to increase the probability of mortality among COVID-19 patients, and different studies have reported varying prevalence of AKI
5,11,12
. The present systematic review aimed to summarize the prevalence and incidence of AKI and mean laboratory tests in COVID-19 patients.
Methods
According to the systematic review and meta-analysis (PRISMA) checklist (see supplementary file S1 for PRISMA checklist),
13
several databases, including PubMed, Scopus, Embase, Web of Science, and MedRxiv, were searched from December 1, 2019, up to July 27, 2020. The search terms were combined using appropriate Boolean operators and adjusted for different databases. The search concepts included subject heading terms/keywords for kidney complications (e.g., "Injury", "Impairment", "Nephro", "Kidney", or "Renal") and SARS-CoV-2 (e.g., "COVID-19" or "Coronavirus"). Supplementary file S2 shows a sample search strategy.
Inclusion criteria and study selection
Studies reporting on the kidney complications of COVID-19 with any design, including case reports, case series, cohorts, and cross-sectional studies, were eligible for this systematic review. However, only cross-sectional and cohort studies were considered for meta-analysis. Non-original studies, such as editorials, letters to the editor, commentaries, and reviews, were excluded from the study. Studies obtained through the electronic database searching were transferred to EndNote software version X8. Two independent co-authors (SHR and AB) completed the title, abstract, and full-text screening process. Any disagreement on the process of selected studies was resolved by discussion with the senior co-author and a nephrologist co-author (ASH and AE).
Data extraction
Data were independently extracted from the eligible studies by two co-authors (NN and SHR). The items considered in data extraction included study characteristics (e.g., first author, publication date, study design, study location, and sample size) and participant characteristics (e.g., age, sex, kidney complications, and laboratory test results).
Quality assessment of the evidence
The Joanna Briggs Institute critical appraisal tool was used to assess the quality of the included studies
14
. This tool evaluates quality with differential items, including 8 items for case report studies, 10 items for case series, 9 items for cross-sectional studies, and 11 items for cohort studies.
Statistical analysis
Descriptive statistics (i.e., mean, median, and standard deviation [SD] for continuous variables and frequency and percentage for categorical variables) were used in this study. Weighted means were utilized to estimate the pooled mean and 95% confidence interval (CI) of laboratory tests. The Metaprop command in Stata software was used to determine the pooled prevalence and incidence of AKI and associated 95% CI of kidney complications. Random-effects meta-analysis was used in the study. The heterogeneity among the included studies was assessed using I2 and Q-statistic. A value of ≥ 50% of I2 and p-value of < 0.1 for the Q-statistic were regarded as considerable heterogeneity. Then, a meta-regression was fitted to assess the potential sources of heterogeneity. For fitting the meta-regression, several variables, namely diagnostic method of COVID-19 (i.e., polymerase chain reaction [PCR] vs. computed tomography [CT] scan and clinical signs), quality of studies (i.e., a quality score of ≥ 4 vs. quality score of < 4), number of study centers (i.e., multi-center vs. single-center), and recruited sample size (i.e., a sample size of > 500 vs. sample size of ≤ 500), were included. Stata software (version 14.2) was used for all statistical analyses. In addition, all comparisons were two-tailed with a threshold p-value of ≤ 0.05 for statistical significance.
Results
Out of the 2,332 retrieved unique records, 51 studies were included in the present systematic review
4,5,15-63
(Figure 1). Four studies were case reports
60-63
, and two studies were case series
28,29
. Furthermore, 27 studies were cohort
4,5,16,17,19,21,24,27,31,33-35,37-39,46,47,49-56,58,59
, and 18 studies were cross-sectional
15,18,20,22,23,25,26,30,32,36,40-45,48,57
. Moreover, 47 and 4 studies reported aggregate-level
4,5,15-59
and individual-level
60-63
information about kidney complications, respectively. Supplementary file S3 shows further details (e.g., population data, location, sex, age, and chronic disease) about the studies included in the present systematic review.
Overall, the studies were carried out on 25,600 patients with COVID-19. The number of patients in different studies was within the range of 1-5,449 patients. Most cases were male (12,294 out of 22,008; 56.0%), and the age range of the participants was within 1 month to 96 years. The SARS-CoV-2 diagnosis was confirmed in 16,598 patients (64.8%) with PCR and 9,002 subjects (35.2%) using clinical signs and CT scans. The most diagnosed comorbidities in patients were hypertension (9,527 out of 22,360; 42.6%), diabetes (5,241 out of 22,360; 23.4%), cardiovascular diseases (2,390 out of 22,360; 10.7%), respiratory diseases (1,886 out of 22,360; 8.4%), and cancer (1,234 out of 22,360; 5.5%). Table 1 tabulates the demographic and clinical characteristics of the patients included in the studies.
Table 1.
Demographic and clinical characteristics of coronavirus disease 2019 patients included in the reviewed studies
|
Characteristics
|
n
|
%
|
| Diagnostic approach (n=25,600) |
|
|
| Only clinical signs and computed tomography scans |
9,002 |
35.2 |
| Confirmed polymerase chain reaction |
16,598 |
64.8 |
| Sex (n=22,008) |
|
|
| Male |
12,294 |
56.0 |
| Female |
9,714 |
44.0 |
| Comorbidity with COVID-19 (n=22,360) |
|
|
| Hypertension |
9,527 |
42.6 |
| Diabetes |
5,241 |
23.4 |
| Cardiovascular diseases |
2,390 |
10.7 |
| Respiratory system diseases |
1,886 |
8.4 |
| Cancer |
1,234 |
5.5 |
| Renal diseases |
1,131 |
5.1 |
| Liver diseases |
436 |
2.0 |
| Cerebrovascular diseases |
388 |
1.7 |
| Autoimmune diseases |
127 |
0.6 |
COVID-19: Coronavirus disease 2019
Quality assessment of included studies
The overall quality of the studies was low. The scores of the case report, case series, cross-sectional, and cohort studies were within the ranges of 2-5 (out of 8 possible points), 2-3 (out of 10 possible points), 1-6 (out of 9 possible points), and 3-7 (out of 11 possible points), respectively. Supplementary file S4 shows further details in this regard.
Pooled prevalence of AKI
The pooled prevalence of AKI was estimated based on the data obtained from 18 cross-sectional studies carried out on 6,505 patients (Figure 2). The pooled prevalence of AKI was estimated as 10.08% (I2=98.56; 95% CI: 4.59, 17.32; P<0.0001).
Pooled incidence of AKI
The pooled incidence of AKI was estimated based on the data obtained from 27 cohort studies conducted on 18,934 patients (Figure 3). The pooled incidence of AKI was estimated as 12.78% (I2=99.27; 95% CI: 7.38, 19.36; P<0.0001).
Biochemical tests
The mean (95% CI) values of SCr, BUN, potassium, and sodium among patients diagnosed with COVID-19 were estimated as 76.10 (69.36, 82.84), 4.60 (4.04, 5.30), 3.94 (3.78, 4.11), and 139.30 (138.26, 140.36) mmol/L, respectively (Table 2).
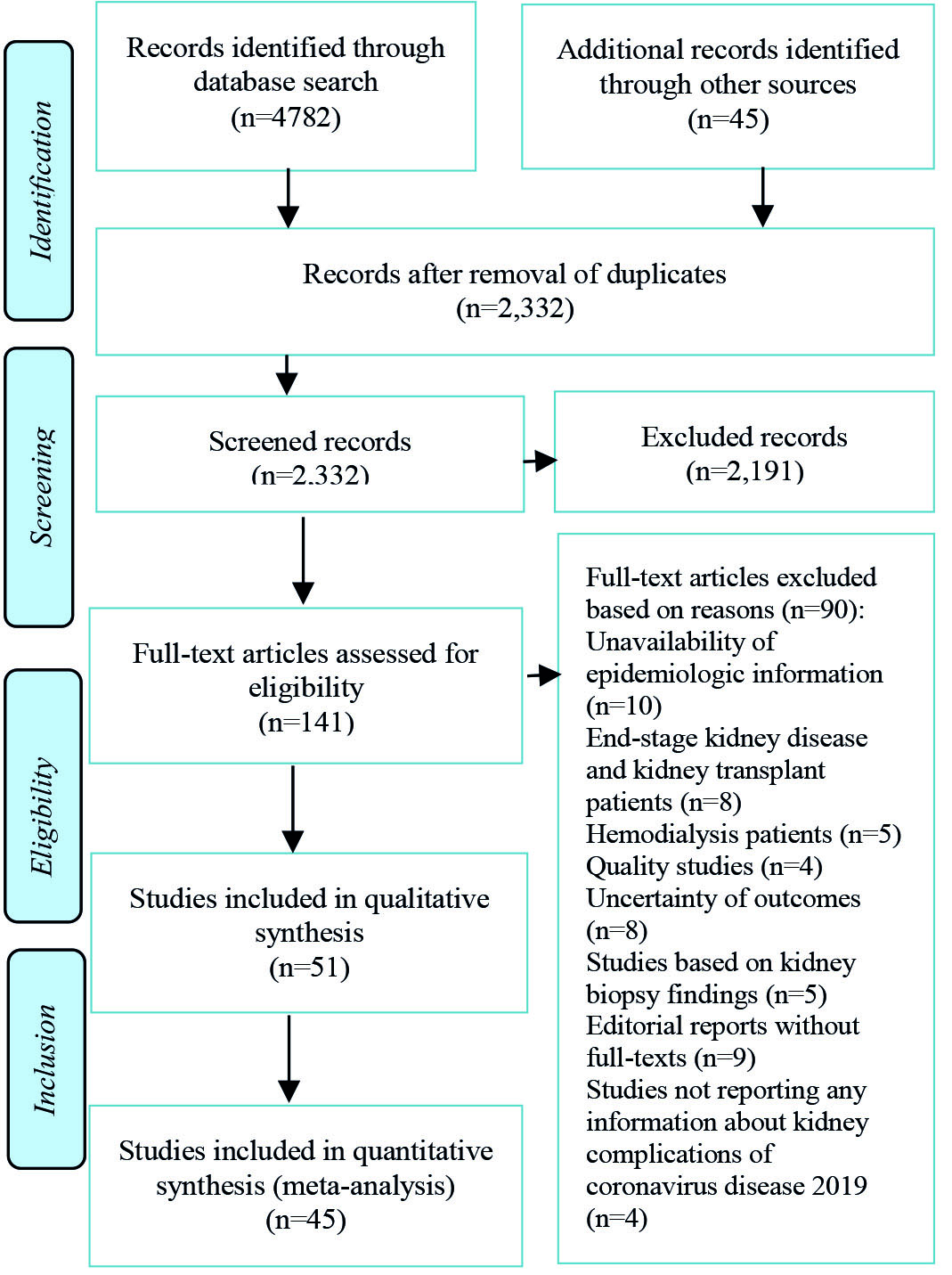
Figure 1.
Flowchart of studies included in the systematic review of coronavirus disease 2019 kidney injury
.
Flowchart of studies included in the systematic review of coronavirus disease 2019 kidney injury
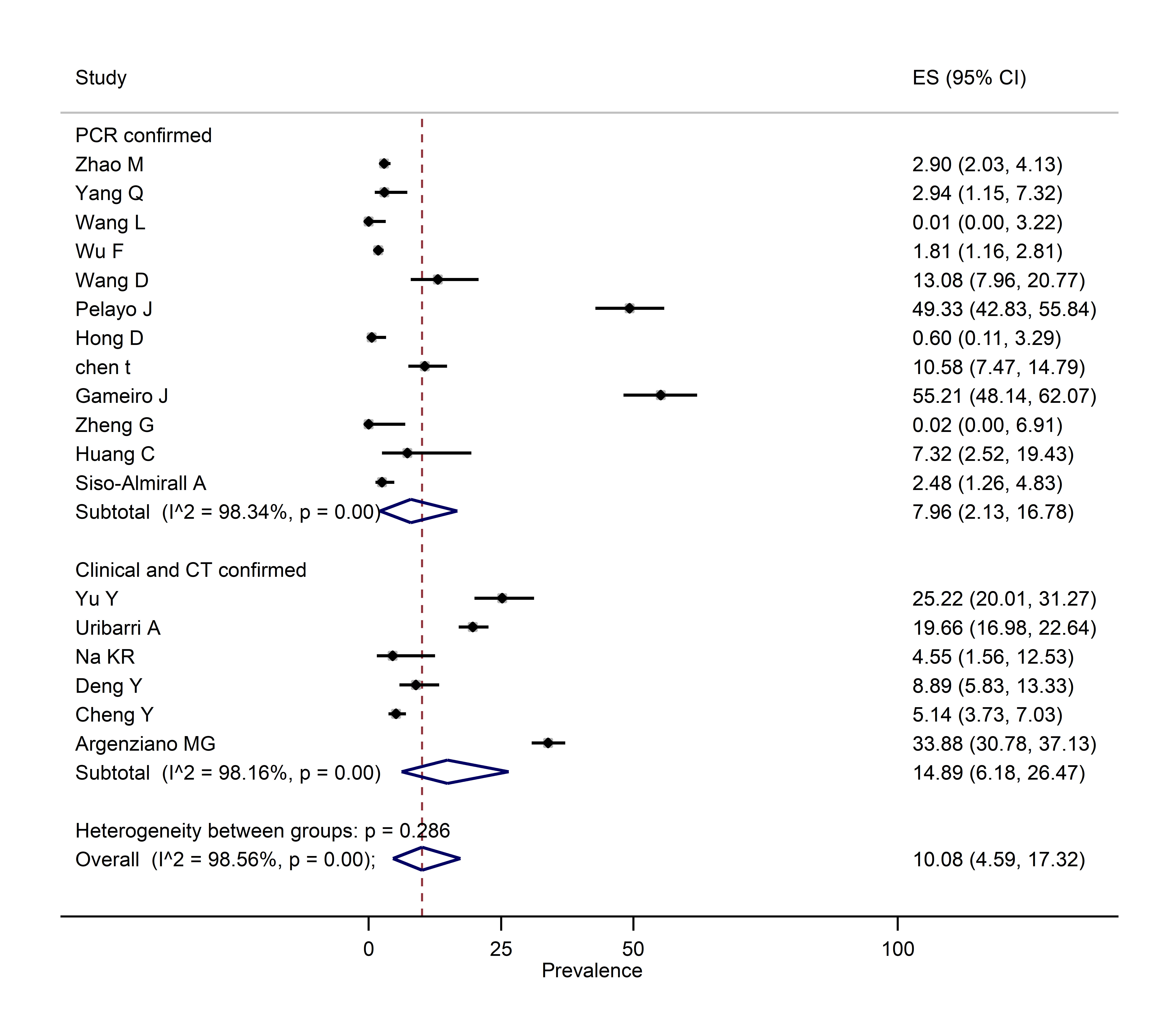
Figure 2.
Pooled prevalence of kidney injury among patients with coronavirus disease 2019
.
Pooled prevalence of kidney injury among patients with coronavirus disease 2019
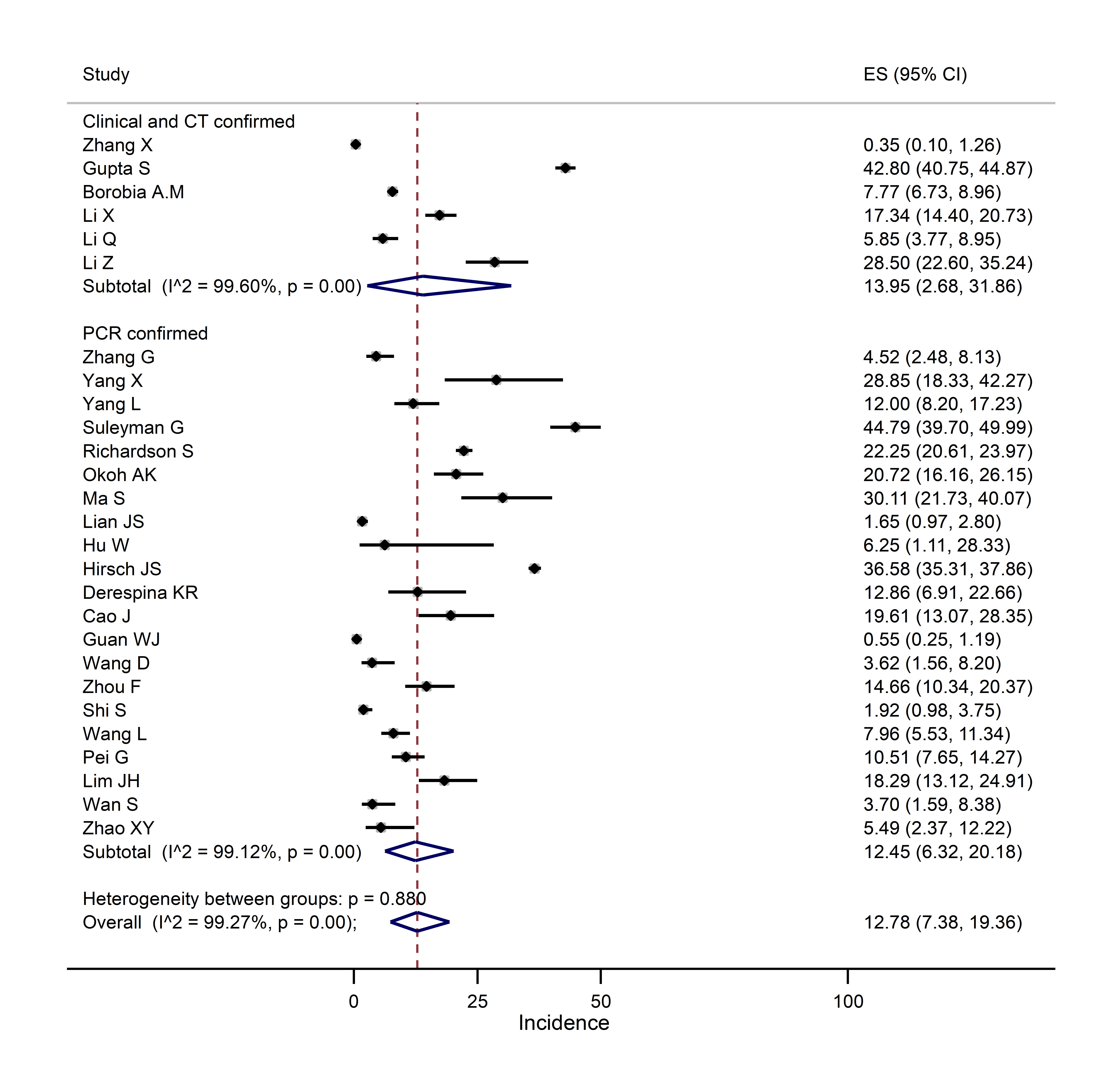
Figure 3.
Pooled incidence of kidney injury among patients with coronavirus disease 2019
.
Pooled incidence of kidney injury among patients with coronavirus disease 2019
Meta-regression
The results of meta-regression did not reveal the significant sources of heterogeneity among the studies included in the present meta-analysis (Table 3).
Discussion
This systematic review and meta-analysis included 51 studies and 25,600 COVID-19 patients. Based on the included evidence, it was estimated that the prevalence and incidence of AKI were about 10% and 12%, respectively. These findings are comparable with previous results varying greatly across different studies. For example, in a study carried out by Pei et al. in China, the incidence of AKI was reported as 4.7% (22 out of 467)
54
. In addition, Cao et al. estimated the incidence of AKI as 19.6% (n=22) among 102 Chinese patients
4
. In the United States, Hirsch et al. studied 5,449 COVID-19 patients and estimated the incidence of AKI as 36.6% (n=1,993)
37
. Moreover, previous systematic reviews have calculated the prevalence of AKI among COVID-19 patients within the range of 3-17%
64,65
.
The AKI has also been reported in previous coronavirus pandemics. For example, Cha et al. reported the prevalence rates of AKI in Middle East Respiratory Syndrome coronavirus and severe acute respiratory syndrome patients to be 26.7% (8 out of 30)
66
and 6.7% (36 out of 536)
67
, respectively. Kidneys have an essential role in drug metabolism. In addition, damages to kidneys and accumulation of drugs could increase toxin accumulation in patients
68,69
. Kidney injuries increase the severity of the disease among COVID-19 patients and need for mechanical ventilation
11,37
. In a recent meta-analysis, the pooled odds ratio for mortality among COVID-19 patients with AKI was reported as 13.3
11
. Paying further attention to kidney injuries in the clinical assessment of patients could help decrease COVID-19-related morbidities and mortalities.
Table 2.
Laboratory tests of coronavirus disease 2019 patients included in the reviewed studies
|
Test
|
Unit
|
Normal range
|
n
|
Mean (95% CI)
|
Range
|
N o. of studies
|
| Serum creatinine |
μmol/L |
70.72-114.92 |
12,887 |
76.1 (69.36, 82.84) |
60-117.6 |
29 |
| Blood urea nitrogen |
μmol/L |
3.1-8.0 |
4,507 |
4.6 (4.04, 5.30) |
3.5-7.34 |
15 |
| Serum potassium |
μmol/L |
3.5-5.3 |
3,541 |
3.94 (3.78, 4.11) |
3.7-4.2 |
9 |
| Serum sodium |
μmol/L |
137-147 |
5,162 |
139.3 (138.26, 140.36) |
137-141.2 |
11 |
| Creatine kinase |
U/L |
50-310 |
6,369 |
87.5 (59.13, 115.93) |
3.85-164 |
16 |
| Procalcitonin |
ng/mL |
0.0-0.5 |
3,472 |
0.09 (0.04, 0.15) |
0.05-0.1 |
6 |
| C-reactive protein |
mg/L |
0-8 |
6,910 |
84.2 (24.97, 143.50) |
3.4-158 |
16 |
Table 3.
Meta-regression of the effect of the factors on the acute kidney injury of coronavirus disease 2019 patients
|
Variable
|
Prevalence
|
Incidence
|
|
Coefficient
|
95% CI
|
P
-value
|
Coefficient
|
95% CI
|
P
-value
|
| Quality score of the included papers (i.e., ≥4 vs. <4) |
0.01 |
-0.17, 0.19 |
0.906 |
0.05 |
-0.07, 0.18 |
0.406 |
| Sample size (i.e., ≤500 vs. >500) |
0.03 |
-0.21, 0.28 |
0.757 |
-0.04 |
-0.20, 0.11 |
0.581 |
| Diagnostic method (i.e., polymerase chain reaction vs. computed tomography scans and clinical signs) |
- 0.08 |
-0.29, 0.13 |
0.433 |
-0.04 |
-0.19, 0.10 |
0.541 |
| Type of study (i.e., multi-center vs. single-center) |
-0.12 |
-0.35, 0.10 |
0.261 |
0.04 |
-0.08, 0.17 |
0.496 |
The weighted mean values of SCr and BUN were 76.1 (range: 60-117.6) and 4.6 (range: 3.5-7.34) mmol/L, respectively. The normal ranges of SCr and BUN are 70.72-114.92 and 3.1-8 mmol/L, respectively. Laboratory tests could be used to diagnose AKI at the early stages of the disease. When used at an appropriate time, laboratory tests can can help reach earlier diagnosis of kidney injuries kidney injuries
11,70
. The BUN and SCr are crucial laboratory tests for the diagnosis of AKI
11,70
and may increase in COVID-19 patients
10
. For example, Zhao et al. showed increased levels of SCr in 11.6% (116 out of 1,000) of COVID-19 patients
15
. Increased BUN and SCr are indeed observed in severe COVID-19 patients in another study
41
. Chen et al. demonstrated BUN levels in deceased patients to be higher than the normal range
42
. However, the weighted mean values of BUN and SCr were within the normal ranges in the included studies. This could be due to the fact that the included studies calculated the weighted mean of BUN and SCr for all COVID-19 patients and not separately for those with AKI. Therefore, the assessment of BUN and SCr in COVID-19 patients with AKI would be informative.
The weighted mean values of potassium and sodium were 3.94 (range: 3.7-4.2) and 139.3 (range: 137-141.2) mmol/L, respectively. The normal ranges of potassium and sodium are 3.5-5.3 and 137-147 mmol/L, respectively. The assessment of the baseline levels of electrolytes can help evaluate the risk of mortality among COVID-19 patients
71
. Sodium may also help predict progression to severe disease in COVID-19 patients
72
. Sodium and potassium levels could be lower in severe COVID-19 cases
73
. For example, Tezcan et al. reported that low baseline sodium was related to higher mortality in COVID-19 patients
71
. In addition, hypernatremia can be a manifestation of COVID-19 and adverse outcomes in COVID-19 cases
74
.
Although sodium and potassium levels are important in COVID-19 patients, the current study showed sodium and potassium levels to be within the normal ranges. This could be due to the fact that the studies measured sodium and potassium only once during the course of the study. Therefore, it is suggested to carry out further studies to measure sodium and potassium levels in the initial admission of patients and continue monitoring the patients’ sodium and potassium levels throughout their hospital admission.
The current study had several limitations. Firstly, the quality of studies included in the meta-analysis was low. Secondly, most studies had a low sample size. Thirdly, the variations between studies could lead to different measurements. Fourthly, the diagnostic methods were the use of PCR in some studies and clinical signs and CT scans in other studies that can be taken into account when interpreting the findings. Nonetheless, the findings of the present study are informative for the enhancement of the identification of AKI among COVID-19 patients.
Conclusions
The prevalence and incidence of AKI seem to be considerable among COVID-19 patients. The BUN, SCr, sodium, and potassium were within the normal ranges. The assessment and monitoring of COVID-19 patients for renal complications and comorbidities can help improve care and health outcomes among COVID-19 patients.
Acknowledgements
MK is a member of the COVID-19 Impact Committee of Pierre Elliott Trudeau Foundation and is supported by the Pierre Elliott Trudeau Foundation Doctoral Scholarship.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This review received no external funding or other supports.
Authors ʼ contributions
All the authors contributed to conceptualization, study design, and data analysis. Screening was completed by SHR and AB. ASH and AE supervised the screening process. Data extraction was carried out by NN and SHR. Data analysis was performed by HSH and MK. NN, HSH, MK, and ASH wrote the first draft of the manuscript. The manuscript was read and approved by all the authors.
Highlights
-
Acute kidney injury is a prevalent complication among coronavirus disease 2019 (COVID-19) patients.
-
Monitoring COVID-19 patients for renal injuries could help improve their health outcomes.
-
Overall, blood urea nitrogen, serum creatinine, sodium, and potassium were within the normal ranges among the included patients in the review.
References
- Del Rio C, Malani PN. COVID-19-New Insights on a Rapidly Changing Epidemic. JAMA 2020; 323(14):1339-40. [ Google Scholar]
- Khalili M, Karamouzian M, Nasiri N, Javadi S, Mirzazadeh A, Sharifi H. Epidemiological characteristics of COVID-19: a systematic review and meta-analysis. Epidemiol Infect 2020; 148:e130. [ Google Scholar]
-
COVID-19 coronavirus pandemic. Worldmeter- real time world statistics; 2020 [cited 20 oct 2020]; Available from: https://www.worldometers.info/.
- Cao J, Tu WJ, Cheng W, Yu L, Liu YK, Hu X. Clinical Features and Short-term Outcomes of 102 Patients with Coronavirus Disease 2019 in Wuhan, China. Clin Infect Dis 2020; 71(15):748-55. [ Google Scholar]
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020; 382(18):1708-20. [ Google Scholar]
- Yao Y, Pan J, Wang W, Liu Z, Kan H, Qiu Y. Association of particulate matter pollution and case fatality rate of COVID-19 in 49 Chinese cities. Sci Total Environ 2020; 741:140396. [ Google Scholar]
-
Fan C, Li K, Ding Y, Lu WL, Wang J. ACE2 expression in kidney and testis may cause kidney and testis damage after 2019-nCoV infection. MedRxiv 2020; 10.1101/2020.02.12.20022418
- Pan XW, Xu D, Zhang H, Zhou W, Wang LH, Cui XG. Identification of a potential mechanism of acute kidney injury during the COVID-19 outbreak: a study based on single-cell transcriptome analysis. Intensive Care Med 2020; 46(6):1114-6. [ Google Scholar]
- Zou X, Chen K, Zou J, Han P, Hao J, Han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med 2020; 14(2):185-92. [ Google Scholar]
- Yang X, Jin Y, Li R, Zhang Z, Sun R, Chen D. Prevalence and impact of acute renal impairment on COVID-19: a systematic review and meta-analysis. Crit Care 2020; 24(1):1-8. [ Google Scholar]
- Hansrivijit P, Qian C, Boonpheng B, Thongprayoon C, Vallabhajosyula S, Cheungpasitporn W. Incidence of acute kidney injury and its association with mortality in patients with COVID-19: a meta-analysis. J Investig Med 2020; 68(7):1261-70. [ Google Scholar]
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020; 323(20):2052-9. [ Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6(7):e1000097. [ Google Scholar]
-
The Joanna Briggs Institute Critical Appraisal tools for use in JBI systematic reviews. Joanna Briggs Institute; 2020 [cited 31 Oct 2020]; Available from: https://joannabriggs.org/critical-appraisal-tools.
- Zhao M, Wang M, Zhang J, Gu J, Zhang P, Xu Y. Comparison of clinical characteristics and outcomes of patients with coronavirus disease 2019 at different ages. Aging 2020; 12(11):10070-86. [ Google Scholar]
- Zhang X, Cai H, Hu J, Lian J, Gu J, Zhang S. Epidemiological, clinical characteristics of cases of SARS-CoV-2 infection with abnormal imaging findings. Int J Infect Dis 2020; 94:81-7. [ Google Scholar]
- Zhang G, Hu C, Luo L, Fang F, Chen Y, Li J. Clinical features and short-term outcomes of 221 patients with COVID-19 in Wuhan, China. J Clin Virol 2020; 127:104364. [ Google Scholar]
- Yu Y, Xu D, Fu S, Zhang J, Yang X, Xu L. Patients with COVID-19 in 19 ICUs in Wuhan, China: a cross-sectional study. Crit Care 2020; 24(1):1-10. [ Google Scholar]
- Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020; 8(5):475-81. [ Google Scholar]
- Yang Q, Xie L, Zhang W, Zhao L, Wu H, Jiang J. Analysis of the clinical characteristics, drug treatments and prognoses of 136 patients with coronavirus disease 2019. J Clin Pharm Ther 2020; 45(4):609-16. [ Google Scholar]
- Yang L, Liu J, Zhang R, Li M, Li Z, Zhou X. Epidemiological and clinical features of 200 hospitalized patients with corona virus disease 2019 outside Wuhan, China: A descriptive study. J Clin Virol 2020; 129:104475. [ Google Scholar]
- Wang L, Li X, Chen H, Yan S, Li D, Li Y. Coronavirus Disease 19 Infection Does Not Result in Acute Kidney Injury: An Analysis of 116 Hospitalized Patients from Wuhan, China. Am J Nephrol 2020; 51(5):343-8. [ Google Scholar]
- Wu F, Zhou Y, Wang Z, Xie M, Shi Z, Tang Z. Clinical characteristics of COVID-19 infection in chronic obstructive pulmonary disease: a multicenter, retrospective, observational study. J Thorac Dis 2020; 12(5):1811-23. [ Google Scholar]
- Suleyman G, Fadel RA, Malette KM, Hammond C, Abdulla H, Entz A. Clinical Characteristics and Morbidity Associated With Coronavirus Disease 2019 in a Series of Patients in Metropolitan Detroit. JAMA Netw Open 2020; 3(6):e2012270. [ Google Scholar]
- Uribarri A, Núñez-Gil IJ, Aparisi A, Becerra-Muñoz VM, Feltes G, Trabattoni D. Impact of renal function on admission in COVID-19 patients: an analysis of the international HOPE COVID-19 (Health Outcome Predictive Evaluation for COVID 19) Registry. J Nephrol 2020; 33(4):737-45. [ Google Scholar]
- Wang D, Yin Y, Hu C, Liu X, Zhang X, Zhou S. Clinical course and outcome of 107 patients infected with the novel coronavirus, SARS-CoV-2, discharged from two hospitals in Wuhan, China. Crit Care 2020; 24(1):1-9. [ Google Scholar]
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020; 323(20):2052-9. [ Google Scholar]
- Xu S, Hu H, Hu Y, Shui H. Clinical features of 62 cases of coronavirus disease 2019 complicated with acute renal injury. Medical Journal of Wuhan University 2020; 41(4):537-41. [ Google Scholar]
- Xiong J, Jiang W, Zhou Q, Hu X, Liu C. Clinical characteristics, treatment, and prognosis in 89 cases of COVID-19. Medical Journal of Wuhan University 2020; 41(4):542-6. [ Google Scholar]
- Pelayo J, Lo KB, Bhargav R, Gul F, Peterson E, DeJoy Iii R. Clinical Characteristics and Outcomes of Community- and Hospital-Acquired Acute Kidney Injury with COVID-19 in a US Inner City Hospital System. Cardiorenal Med 2020; 10(4):223-31. [ Google Scholar]
- Okoh AK, Sossou C, Dangayach NS, Meledathu S, Phillips O, Raczek C. Coronavirus disease 19 in minority populations of Newark, New Jersey. Int J Equity Health 2020; 19(1):1-8. [ Google Scholar]
- Na KR, Kim HR, Ham Y, Choi DE, Lee KW, Moon JY. Acute Kidney Injury and Kidney Damage in COVID-19 Patients. J Korean Med Sci 2020; 35(28):e257. [ Google Scholar]
- Ma S, Lai X, Chen Z, Tu S, Qin K. Clinical characteristics of critically ill patients co-infected with SARS-CoV-2 and the influenza virus in Wuhan, China. Int J Infect Dis 2020; 96:683-7. [ Google Scholar]
- Lian JS, Cai H, Hao SR, Jin X, Zhang XL, Zheng L. Comparison of epidemiological and clinical characteristics of COVID-19 patients with and without Wuhan exposure history in Zhejiang Province, China. J Zhejiang Univ Sci B 2020; 21(5):369-77. [ Google Scholar]
- Hu W, Chen X, He B, Yuan S, Zhang X, Wu G. Clinical characteristics of 16 patients with COVID-19 infection outside of Wuhan, China: a retrospective, single-center study. Ann Transl Med 2020; 8(10):642. [ Google Scholar]
- Hong D, Long L, Wang AY, Lei Y, Tang Y, Zhao JW. Kidney manifestations of mild, moderate and severe coronavirus disease 2019: a retrospective cohort study. Clin Kidney J 2020; 13(3):340-6. [ Google Scholar]
- Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int 2020; 98(1):209-18. [ Google Scholar]
- Gupta S, Hayek SS, Wang W, Chan L, Mathews KS, Melamed ML. Factors Associated With Death in Critically Ill Patients With Coronavirus Disease 2019 in the US. JAMA Intern Med 2020; 15:e203596. [ Google Scholar]
- Derespina KR, Kaushik S, Plichta A, Conway EE, Jr Jr, Bercow A, Choi J. Clinical Manifestations and Outcomes of Critically Ill Children and Adolescents with Coronavirus Disease 2019 in New York City. J Pediatr 2020; 226:55-63. [ Google Scholar]
- Deng Y, Liu W, Liu K, Fang YY, Shang J, Zhou L. Clinical characteristics of fatal and recovered cases of coronavirus disease 2019 in Wuhan, China: a retrospective study. Chin Med J (Engl) 2020; 133(11):1261-7. [ Google Scholar]
- Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int 2020; 97(5):829-38. [ Google Scholar]
- Chen T, Wu D, Chen H, Yan W, Yang D, Chen G. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ 2020; 368:m1091. [ Google Scholar]
-
Gameiro J, Fonseca JA, Oliveira J, Marques F, Bernardo J, Costa C, et al. Acute kidney injury in hospitalized patients with COVID-19 2020; 10.21203/rs.3.rs-39131/v1
- Argenziano MG, Bruce SL, Slater CL, Tiao JR, Baldwin MR, Barr RG. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: retrospective case series. BMJ 2020; 369:m1996. [ Google Scholar]
- Zheng G, Wang B, Zhang H, Xie C, Zhang Y, Wen Z. Clinical characteristics of acute respiratory syndrome with SARS-CoV-2 infection in children in South China. Pediatr Pulmonol 2020; 55(9):2419-26. [ Google Scholar]
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020; 323(11):1061-9. [ Google Scholar]
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020; 395(10229):1054-62. [ Google Scholar]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395(10223):497-506. [ Google Scholar]
- Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol 2020; 5(7):802-10. [ Google Scholar]
- Wang L, He W, Yu X, Hu D, Bao M, Liu H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J Infect 2020; 80(6):639-45. [ Google Scholar]
- Borobia AM, Carcas AJ, Arnalich F, Álvarez-Sala R, Monserrat-Villatoro J, Quintana M. A Cohort of Patients with COVID-19 in a Major Teaching Hospital in Europe. J Clin Med 2020; 9(6):1733. [ Google Scholar]
- Li X, Xu S, Yu M, Wang K, Tao Y, Zhou Y. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J Allergy Clin Immunol 2020; 146(1):110-8. [ Google Scholar]
-
Li Q, Ling Y, Zhang J, Li W, Zhang X, Jin Y, et al. Clinical characteristics of SARS-CoV-2 infections involving 325 hospitalized patients outside Wuhan 2020; 10.21203/rs.3.rs-18699/v1
- Pei G, Zhang Z, Peng J, Liu L, Zhang C, Yu C. Renal Involvement and Early Prognosis in Patients with COVID-19 Pneumonia. J Am Soc Nephrol 2020; 31(6):1157-65. [ Google Scholar]
- Lim JH, Park SH, Jeon Y, Cho JH, Jung HY, Choi JY. Fatal Outcomes of COVID-19 in Patients with Severe Acute Kidney Injury. J Clin Med 2020; 9(6):1718. [ Google Scholar]
- Wan S, Xiang Y, Fang W, Zheng Y, Li B, Hu Y. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J Med Virol 2020; 92(7):797-806. [ Google Scholar]
- Sisó-Almirall A, Kostov B, Mas-Heredia M, Vilanova-Rotllan S, Sequeira-Aymar E, Sans-Corrales M. Prognostic factors in Spanish COVID-19 patients: A case series from Barcelona. PloS One 2020; 15(8):e0237960. [ Google Scholar]
-
Li Z, Wu M, Yao J, Guo J, Liao X, Song S, et al. Caution on kidney dysfunctions of COVID-19 patients. medRxiv 2020; 10.2139/ssrn.3559601
- Zhao XY, Xu XX, Yin HS, Hu QM, Xiong T, Tang YY. Clinical characteristics of patients with 2019 coronavirus disease in a non-Wuhan area of Hubei Province, China: a retrospective study. BMC Infect Dis 2020; 20(1):1-8. [ Google Scholar]
- Zhou B, She J, Wang Y, Ma X. Venous thrombosis and arteriosclerosis obliterans of lower extremities in a very severe patient with 2019 novel coronavirus disease: a case report. J Thromb Thrombolysis 2020; 50(1):229-32. [ Google Scholar]
- Sise ME, Baggett MV, Shepard JO, Stevens JS, Rhee EP. Case 17-2020: A 68-Year-Old Man with Covid-19 and Acute Kidney Injury. N Engl J Med 2020; 382(22):2147-56. [ Google Scholar]
- Tuma J, Neugebauer F, Rohacek M, Serra A. [Renal Monomorphology in COVID-19 with Acute Renal Insufficiency]. Praxis 2020; 109(9):731-5. [ Google Scholar]
- Nalesso F, Garzotto F, Cattarin L, Gobbi L, Qassim L, Sgarabotto L. A Continuous Renal Replacement Therapy Protocol for Patients with Acute Kidney Injury in Intensive Care Unit with COVID-19. J Clin Med 2020; 9(5):1529. [ Google Scholar]
- Ng JJ, Luo Y, Phua K, Choong A. Acute kidney injury in hospitalized patients with coronavirus disease 2019 (COVID-19): A meta-analysis. J Infect 2020; 81(4):647-79. [ Google Scholar]
- Robbins-Juarez SY, Qian L, King KL, Stevens JS, Husain SA, Radhakrishnan J. Outcomes for Patients With COVID-19 and Acute Kidney Injury: A Systematic Review and Meta-Analysis. Kidney Int Rep 2020; 5(8):1149-60. [ Google Scholar]
- Cha RH, Joh JS, Jeong I, Lee JY, Shin HS, Kim G. Renal Complications and Their Prognosis in Korean Patients with Middle East Respiratory Syndrome-Coronavirus from the Central MERS-CoV Designated Hospital. J Korean Med Sci 2015; 30(12):1807-14. [ Google Scholar]
- Chu KH, Tsang WK, Tang CS, Lam MF, Lai FM, To KF. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int 2005; 67(2):698-705. [ Google Scholar]
-
Brienza N, Puntillo F, Romagnoli S, Tritapepe L. Acute kidney injury in coronavirus disease 2019 infected patients: a meta-analytic study. Blood Purif 2020; 10.1159/000509274
- Leblanc M, Kellum JA, Gibney RT, Lieberthal W, Tumlin J, Mehta R. Risk factors for acute renal failure: inherent and modifiable risks. Curr Opin Crit Care 2005; 11(6):533-6. [ Google Scholar]
- Chen YS, Chou CY, Chen ALP. Early prediction of acquiring acute kidney injury for older inpatients using most effective laboratory test results. BMC Med Inform Decis Mak 2020; 20(1):1-11. [ Google Scholar]
- Tezcan ME, Dogan Gokce G, Sen N, Zorlutuna Kaymak N, Ozer RS. Baseline electrolyte abnormalities would be related to poor prognosis in hospitalized coronavirus disease 2019 patients. New Microbes New Infect 2020; 37:100753. [ Google Scholar]
- Duan J, Wang X, Chi J, Chen H, Bai L, Hu Q. Correlation between the variables collected at admission and progression to severe cases during hospitalization among patients with COVID-19 in Chongqing. J Med Virol 2020; 92(11):2616-22. [ Google Scholar]
- Lippi G, South AM, Henry BM. Electrolyte imbalances in patients with severe coronavirus disease 2019 (COVID-19). Ann Clin Biochem 2020; 57(3):262-5. [ Google Scholar]
- Zimmer MA, Zink AK, Weißer CW, Vogt U, Michelsen A, Priebe HJ. Hypernatremia-A manifestation of COVID-19: a case series. A A Pract 2020; 14(9):e01295. [ Google Scholar]