J Res Health Sci. 21(1):e00504.
doi: 10.34172/jrhs.2021.42
Review Article
Sexual and Reproductive Health Challenges in Temporary Marriage: A Systematic Review
Farzaneh Valizadeh 1, Abolfazl Mohammadbeigi 2, Reza Chaman 3, Fatemeh Kashefi 4, Ali Mohammad Nazari 5, Zahra Motaghi 6, *
Author information:
1Student Research Committee, Shahroud University of Medical Sciences, Shahroud, Iran
2Research Center for Environmental Pollutants, Department of Epidemiology, Faculty of Health, Qom University of Medical Sciences, Qom, Iran
3Department of Epidemiology, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran
4Department of Family Health, Deputy of Health, Mazandaran University of Medical Sciences, Mazandaran, Iran
5Department of Reproductive Health, School of Nursing and Midwifery, Shahroud University of Medical Sciences, Shahroud, Iran
6Reproductive Health Department, School of Nursing and Midwifery, Shahroud University of Medical Sciences, Shahroud, Iran
* Correspondence: Zahra Motaghi (PhD) Tel: +98 23 32395054 Fax: +98 23 32395009 E-mail:
zhrmotaghi@yahoo.com
Abstract
Background: Temporary marriage is a legal form of marriage in Shia Islam allowing a man and a woman to become married in a fixed period of time. This review was conducted to identify the potential effects of temporary marriage on the sexual and reproductive health of women.
Study design: A systematic review
Methods: Electronic databases, including Web of Knowledge, Embase, PubMed, Scopus, ScienceDirect, PsycINFO, ProQuest, IranMedex, Scientific Information Database (SID), and Magiran, were searched up to October 2020 to identify the studies carried out on sexual and reproductive health challenges in temporary marriage. All the selected articles were assessed for eligibility according to their titles and abstracts.
Results: During the search on articles published within 1995 to October 2020, 1,802 relevant records were identified, and after evaluation 30 full-text papers were included in the present systematic review. Out of the 34,085 study participants in the selected studies, 3,547 subjects had temporary marriage who were studied under six different categories, namely (1) sexually transmitted infections (STIs)/human immunodeficiency viruses, (2) early child marriage, (3) unplanned pregnancy and induced abortion, (4) violence, (5) psychosocial disorders, and (6) other issues. Individuals with temporary marriage are vulnerable and need to have easy access to health education and sexual and reproductive health services in a safe and unprejudiced environment. Ignoring the aforementioned facts will cause serious public health problems, especially for women from a lower socioeconomic background.
Conclusions: In the current situation with under-reporting of temporary marriage-related events due to social stigma and absence of quality services in sexual and reproductive health, women with temporary marriage are under the additional risk of STIs, unwanted pregnancy, abortion, and violence.
Keywords: Induced Abortion, Sexually Transmitted Diseases, Unplanned Pregnancy, Temporary Marriage, Violence
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Citation: Valizadeh F, Mohammadbeigi A, Chaman R, Kashefi F, Nazari AM, Motaghi Z. Sexual and Reproductive Health Challenges in Temporary Marriage: A Systematic Review. J Res Health Sci. 2021; 21(1): e00504.
Introduction
Temporary marriage or Mut’ah or Sigheh is a temporal contract between a man and an unmarried woman in which the couple agrees to be married for a specified length of time (from 1 hour to 99 years) for a fixed sum of money or gift that is given to the woman. Although temporary marriage is a legal and legitimate form of marriage and permitted in Shia Islam, it is looked down upon by self-respecting families and is not acceptable in the community. Temporary marriage is legitimate in Iranian civil law (Principles: 1075, 1095-98)
1-4
. Due to no necessity to register a temporary marriage and secrecy and social stigma of being involved in such type of marriage, no valid statistics are available on temporary marriage. However, unofficial sources report that the number of temporary marriages has been rising
5
.
Temporary marriage and other sorts of nonconventional marriages are observed within the extended Middle East and North Africa (EMENA) region, including Iran. Consistent with the results of previous studies, the EMENA region may be a region with the youngest population, where globalization, migration, information technology, and political changes are contributing to the reshaping of sexual behaviors and marriage
6,7
. Countries with legal temporary marriage (e.g., Iran, Lebanon, and Iraq) are facing social and health concerns related to temporary marriage that may affect public sexual and reproductive health. Issues affecting temporary marriage health-related topics include under-reporting temporary marriage due to social stigma and limited reproductive and sexual health services (particularly sex protection and family planning services)
8,9
.
In war-torn countries, children are even more at risk of under-aged forced and temporary marriage due to economic and social problems
10,11
. This group of girls has contracted sexually transmitted infections (STIs) and about 14% of them were already human immunodeficiency viruses (HIV) positive
12
. Some studies showed that the phenomenon of temporary marriage plays a role in the promotion of early child marriages in Iran
13
.
These nonpermanent and often secret marriages are often a source of severe oppression and no sexual freedom or socioeconomic independence
14
. However, according to several experts, although temporary marriage is a legitimate response to young individuals’ needs due to economic and social barriers to conventional marriage, it may threaten women’s health by increasing the risk of STIs/HIV, early child marriage, unwanted pregnancies, illegal abortions, coercion, and loss of family and social supports
7,9,14
.
In addition, due to its secrecy, temporary marriage does not provide women with legal protection against different types of abuse that most married women seek. This causes wives with temporary marriage to experience abuse, anxiety, limited social interactions, fewer social opportunities (i.e., occupational and educational opportunities), and therefore lower quality of life. Most published studies have been qualitative or based on legal jurisprudential aspects of temporary marriage. Health-oriented studies are paid less attention as they are scattered and discrete. Therefore, it is necessary to systematically review the health-oriented studies to provide a better and more realistic view of the effects of temporary marriage on women’s health.
Error! Bookmark not defined. Methods
Protocol and registration
The present systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA) statement. The protocol of systematic reviews is usually registered in the international prospective register of systematic reviews. This study was submitted to PROSPERO (receipt code: 226070).
Search strategy and study selection criteria
A comprehensive search was performed to identify any cross-sectional, cohort, or case-control studies investigating sexual and reproductive health challenges in women with temporary marriage. Accordingly, several sources, including Web of Science, Scopus, PubMed, PsycINFO, ProQuest, ScienceDirect, Magiran, Scientific Information Database (SID), IranMedex, and MedLib, were searched. Five sets of related Medical Subject Headings (MeSH) and nonMeSH terms in titles, abstracts, or keywords were used, including (“Temporary Marriage” OR “Sigheh” OR “Mut’ah”, OR “Short-form Marriage” OR “Short-term Marriage” OR “Nikah Mutʼah”) AND (“STD” OR “Sexually Transmitted Disease” OR “STI” OR “Sexually Transmitted Infection” OR “STI/ HIV” OR ”Venereal Diseases”) OR (“Reproductive Health”) OR (“Abortion” OR “Pregnancy Loss” OR “Miscarriage”) OR (“Violence” OR “Domestic Violence” OR “Spousal Abuse”, OR “Intimate Partner Violence”, OR “Sexual Violence” OR “Sexual Abuse” OR “Sex Offense” OR “Coercion”) OR (“Unplanned pregnancy” OR “Unintended Pregnancy” OR “Unwanted Pregnancy” OR “Mistimed Pregnancy”), and their equivalent in MeSH. Furthermore, a combination of these keywords was used for article extraction and searched for articles published up to October 2020. The search strategy was performed using Boolean operators (AND, OR). Two authors independently reviewed the articles and discrepancies were resolved by discussing with the third author. The reference lists of related articles were also manually reviewed for other possibly relevant studies that were not identified through the electronic search strategy.
Inclusion and exclusion criteria
Observational, prospective or retrospective cohort, case-control, and cross-sectional studies investigating the temporary marriage were included in the present review. Duplicate publications or studies using the same sample were excluded. Studies not reporting sample size, review studies, qualitative studies, editorials, letters to the editors, commentaries, expert opinions, case series, case studies, brief reports, and book chapters were not included in the present systematic review and meta-analysis.
Data extraction and quality assessment
Two independent authors (F.V and A.MB) extracted several characteristics from the included studies, such as author’s name, year of publication, study state/province, study sample size, and number of temporary marriages of individuals. Any disagreement between the two reviewers was resolved through discussion with the senior author (Z.M). The Newcastle-Ottawa scale (NOS) is one of the most known scales for the assessment of the quality and risk of bias in observational studies. The NOS checklist is assigned up to a maximum of nine points for the least risk of bias in three domains, namely selection of study groups (4 points), comparability of groups (2 points), and ascertainment of exposure and outcomes (3 points) for these studies, respectively. Based on the NOS, the quality of the articles was rated within a range of 0-9. Total scores were categorized into three following groups:
-
(0-3): Very high risk of bias
-
(4-6): High risk of bias
-
(7-9): Low risk of bias
15,16
According to some sources for data retention, studies with lower than 5 points
17
or some studies with a score lower than the mean score of studies
18
identified as representing a high risk of bias were considered low quality and excluded
17,18
. In this study, based on the NOS, studies with lower than 5 points were regarded as low quality and excluded. For each article, some information, including authors, objectives, places, sample sizes, study types, statistical analyses, and main results, were extracted. Each study was independently assessed by three authors (F.V, A.MB, and F.K) and then the data were independently extracted. Other authors (Z.M, R.C, and A.M.N.) were considered an arbiter to resolve any disagreements.
Results
Included studies
As illustrated in Figure 1, according to the PRISMA flowchart, 1,802 studies which were reported by eight countries were extracted through searching. Out of these 1,802 studies, 1772 papers were excluded after reviewing the titles and abstracts, then full text of the remaining articles were assessed. Finally, 30 studies met the eligibility criteria and were included in the current systematic review. In the present study, no study was identified on the health consequences of temporary marriage, except for 28 Iranian articles and 2 articles on Syrian refugees in Jordan. There were 30 relevant articles that were published within 1998 to October 2020 with 34,085 study participants, out of whom 3,547 individuals had temporary marriage. According to these studies, the rate of temporary marriage was various in different areas and groups. Table 1 tabulates the main characteristics of the included studies. The selected (n=30) articles were published within 1998 to October 2020 in six different categories, namely 1) STIs/HIV, 2) early child marriage, 3) abortion and unintended pregnancy, 4) violence and coercion, 5) psychosocial disorders, and 6) others issues.
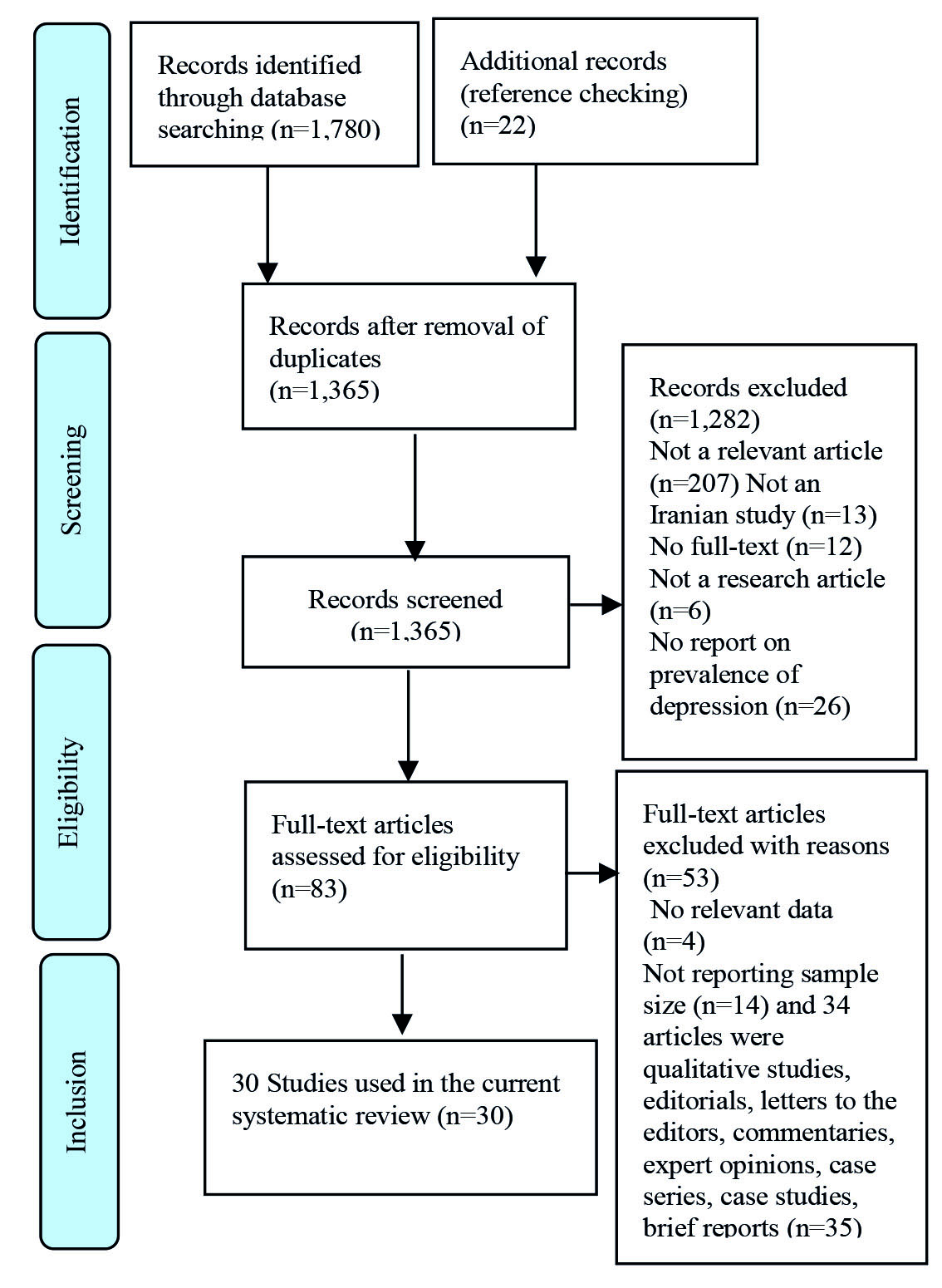
Figure 1.
PRISMA flowchart of studies included and excluded at each stage of screening
.
PRISMA flowchart of studies included and excluded at each stage of screening
STIs/HIV
Through searching, 18 articles were identified on STIs/HIV among individuals with temporary marriage. Based on the sampling methods, these articles were divided into two study groups. In the first group (n=5; with a sample size of 8,293 individuals), the studied population consisted of individuals of reproductive age. The results of studies carried out by Khani et al. and Rostami et al. on women referring to health care centers in northern cities of Iran, Hassani et al. on volunteers for marriage in Bandar Abbas, Iran, Shokoohi et al. on individuals within the age range of 15-29 years at a national level, and Kazem Mohammad et al. on male adolescent aged 15-18 years in Tehran, Iran, showed that temporary marriage experience and unprotected sex were within the ranges of 1.5-14% and 50-80%, respectively
19-23
. In the second group (n=13), high-risk behavior groups, including female sex workers and male intravenous-drug users, with a sample size of 7,691, were studied at a national level. The results indicated that a significant percentage of individuals in these high-risk groups had at least a temporary marriage and the rates of unprotected sex and STIs were very high
24-36
. The results of logistic regression in a study performed by Fallahi et al. demonstrated that the risk of acquiring STIs increases 4.3 times in homeless women with temporary marriage, compared to that reported for homeless women without temporary marriage (OR=4.33; OR=3; 95% CI: 1.39-13.49; P=0.010)
28
. In a study conducted by Shaditalab et al., it was estimated that 30% of female addicts in Tehran had multiple temporary marriages
37
. In addition, a study carried out on Syrian refugee women showed that 11.5% of women with temporary marriage reported having STIs and two-third of them declared that their spouses refused to use a condom during their sexual intercourse
38
.
Early child marriage
The International Planned Parenthood Federation defined early child marriage as any marriage under the age of 18 years
12
. Iran Demos and Health Statistics states that in some parts of Iran temporary marriage among under-age girls (not reaching the legal age for marriage) is common. In other words, temporary marriage leads to child abuse by spouses
13
. In searching with the related keywords, a study conducted on temporary marriage in young females among Syrian refugees was identified. According to the results, young-female and older Syrian refugees were sexually exploited through the temporary marriage system. In 2013, approximately 25% of the registered temporary marriages of Syrians in Jordan involved Syrian adolescents within the age range of 15-17 years and the majority of these children were girls
39
.
Unplanned pregnancy and abortion
Unwanted pregnancies and their complications are the most important factors with a negative impact on women’s health. Studies carried out by Cheraghi et al., Motaghi et al., and Francome on the complications of women’s health with temporary marriage indicated that Nikah mutʼah makes the institutionalization of sex without commitment possible. In addition, mutʼah is considered one of the most common predictive factors of unwanted pregnancies and unsafe abortions that is usually due to a men’s lack of participation in using family planning methods
40-42
. Abortion is a multidimensional phenomenon with several social, legal, and religious implications
43
. The results of a study conducted by Pourreza and Batebi showed that 6% of women referring to medical centers for abortion had temporary marriage and were at risk for physical and mental complications due to a lack of sociocultural acceptance
44
. Moreover, the results of a study carried out by Jamshidi and Saroukhani in obstetrics and gynecology clinics of Alborz province, Iran, indicated that 33% of women with temporary marriage had a history of unwanted pregnancy, 88% of whom had abortions and 22.7% of whom were left by temporary husbands
45
. Similarly, a study performed by Nokhodian et al. in Isfahan, Iran, showed that 36% of female prisoners with temporary marriage had a history of abortion
27
. In this regard, the results of a study performed by Jahanfar et al. on women referring for antenatal care demonstrated that 0.7% of them were women with temporary marriage
46
. The results showed that most women with temporary marriage were reluctant to continue the pregnancy because their husbands abandoned them and they reported different supportive problems.
Table 1.
Main characteristics of the studies included in the present systematic review
|
No.
|
Author, y ear
|
Target group, country
|
Age (yr )
|
Sampling method
|
Type of study
|
Results
|
N OS
|
|
STIs/HIV
|
| 1 |
Zargooshi et al, 2002
31
|
100 male gonorrhea patients, Iran |
19-35 |
Convenience sampling |
Cohort |
24 men became infected by temporary wives (100% - temporary marriage-individual) and78% of males had unprotected sex (n=19) |
7 |
| 2 |
Ghanbarzadeh el al, 2005
33
|
200 women prisoners, Iran |
16-73 |
Census method |
Cross-Sectional |
22 women reported that they had temporary marriage and prevalence of STI among them was 11%. |
5 |
| 3 |
Kazem Mohamad et al, 2007
22
|
1,385 adolescent males, Iran |
15-18 |
Cluster sampling |
Cross-Sectional |
198 (14.2%) adolescent boys had sexual contact with women with temporary marriage 164 (37%) of their partners had protected sex. |
9 |
| 4 |
Tehrani et al,
2008
26
|
At-risk-1005 Young, Iran |
15-40 |
Segmentation method |
Cross-Sectional |
379 (37%) youths had temporary marriage; prevalence of STIs and unprotected sex were 34% and 35.1%, respectively. |
8 |
| 5 |
Kassaian et al, 2011
29
|
100 female sex workers, Iran |
18-42 |
Convenience sampling |
Cross-sectional |
34 female sex workers reported having temporary marriage; 16% of their partners had protected sex and 9 % of them had HCVAb+ |
6 |
| 6 |
Nokhodian et al,
2012
27
|
163 women prisoners, Iran |
15-45 |
Census method |
Cross-sectional |
29 of female prisoners reported temporary marriage and having HCVAb (7%). |
7 |
| 7 |
Alipour et al,
2013
27
|
452 male and female intravenous-drug abusers, Iran |
20-41 |
Convenience sampling |
Cross-sectional |
88 (%19) subjects reported having temporary marriage; %27 of their partners had protected sex. |
8 |
| 8 |
Hassani Azad et al, 2016
23
|
600 volunteers for marriage, Iran |
19-34 |
Available sampling |
Cross-sectional |
12 men and women reported having temporary marriage 55% of whom had unprotected sex and did not have HIV positive test. |
7 |
| 9 |
Shokoohi et al, 2016
24
|
1,005 female sex workers, Iran |
25–34 |
Facility-based sampling |
Cross-sectional |
200 had temporary marriage; 17% of them were HIV-positive and 64% of them had received free condoms. |
8 |
| 10 |
Shokoohi et l, 2016
21
|
5,395 youths, Iran |
15-29 |
Multistage cluster sampling |
Cross-sectional |
562 youths had temporary marriage; 21.8% of their partners had protected sex. |
9 |
| 11 |
Rostami et al, 2017
20
|
400 women referring to health centers, Iran |
20-36 |
Available sampling |
Cross-sectional |
12 of women referring to health centers had temporary marriage; 70% and 65% of them had unprotected sex and STIs, respectively. |
7 |
| 12 |
ShahEsmaili et al, 2017
32
|
1,337 female sex workers, Iran |
23-44 |
Facility-based sampling |
Cross-sectional |
134 (10%) FSW reported having temporary marriage; 50% and 32.9% of women with temporary marriage had STI and protected sex, respectively; the most prevalent STIs was human papillomavirus, and prevalence of HIV was 2.0%. |
8
|
13
|
Rezaianzadeh et al, 2017
25
|
1,052 individuals infected with HIV, Iran |
25-49 |
Census method sampling |
Historical cohort |
16 (1.5%) HIV+ subjects reported having temporary marriage.
|
6 |
| 14 |
Khoei et al, 2017
35
|
300 Iranian male drug users, Iran |
31-38 |
Segmentation method |
Cross-sectional |
5 (1.5%) drug users had a history of temporary marriage 80% of whom had high-risk sexual behaviors. |
8 |
| 15 |
Khani et al, 2018
19
|
514 female sex workers, Iran |
23-38 |
Multistage sampling |
Cross-sectional |
13 (2.6%) women had the experience of temporary marriage 85% of whom did not use a condom; 56% of them had STIs. |
7 |
| 16 |
Behzadi et al, 2018
30
|
71 HIV-infected women, Iran |
27-36 |
Convenience sampling |
Cross-sectional |
5 (7%) women reported having temporary marriage; 21% and %77 of women with temporary marriage had protected sex and other STIs. |
8 |
| 17 |
Asadi et al, 2018
34
|
184 female sex workers, Iran |
23-40 |
Convenience sampling |
Cross-sectional |
27 FSW reported having temporary marriage 56% of whom had unprotected sex. |
7 |
| 18 |
Fallahi et al, 2019
28
|
241 homeless women
in DIC, Iran
|
20-48 |
Quota sampling |
Cross-sectional |
57 (23.5%) homeless women reported having temporary marriage; 23% and 22% of women with temporary marriage had STIs and protected sex, respectively; the results of logistic regression showed that the risk of acquiring STIs increases 4.3 times in homeless women with temporary marriage, compared to that of homeless women without temporary marriage (OR=4.33; OR=3; 95% CI: 1.39-13.49; P=0.01). |
8 |
| 19 |
Dua’ Al-Maharma et al, 2019
38
|
523 Syrian refugee women,
Jordan
|
16-44 |
Proportional quota sampling |
Cross-sectional |
11.5% of Syrian refugee women with temporary marriage (n=60) had STIs and 67% of them had unprotected sex. |
7 |
|
Early child marriage
|
| 20 |
Spencer RA, et al 2015
39
|
2,936 registered Syrian temporary marriages, Jordan |
15-17 |
Census method |
Cross-sectional |
Syrian young girls and women are sexually exploited through a temporary marriage; 25% of them (n=735) involved Syrian girls within the age range of 15-17 years. |
6 |
|
Unintended pregnancy
|
| 21 |
Jamshidi et al, 2016
45
|
53 women with temporary marriage, Iran |
21-40 |
Convenience sampling |
Cross-sectional |
33% of women with temporary had unintended pregnancy; 88% of them aborted their pregnancy. |
7 |
| 22 |
PourReza et al, 2011
44
|
278 women with abortion, Iran |
15-49 |
Convenience sampling |
Cross-sectional |
6% (17) of women who had abortion experiences were women with temporary marriage. |
8 |
| 23 |
Jahanfar et al, 1998
46
|
3,028 women seeking prenatal care,
Iran
|
18-41 |
Proportion stratification |
Cross-sectional |
Only 0.7 % of subjects reported having temporary marriage. |
7 |
| Repeated |
Nokhodian et al,
2012
27
|
163 female prisoners, Iran |
15-45 |
Census method |
Cross-sectional |
29 (18%) female prisoners reported temporary marriage; 36% of women with temporary marriage had an abortion. |
8 |
|
Violence
|
| 24 |
Eslamloo et al, 2006
48
|
261 women with spousal abuse referring to Urmia Forensic Medicine, Iran |
21-46 |
Census method |
Cross-sectional |
60 (23 (%women complaining to forensic medicine were women with temporary marriage;
Adjusted OR: 4.6 (CI 95%:1.25-17.7; P: 0.01) of violence in temporary marriage in comparison to that in permanent marriage
|
7 |
| 25 |
Khoei et al, 2015
50
|
120 female drug users, Iran |
26-45 |
Multistage sampling |
Cross-sectional |
0.8% of female drug users reported having temporary marriage and experienced high rates of domestic violence. |
8 |
| 26 |
Rahmani et al, 2020
49
|
1,337 femal sex workers, Iran |
20-45 |
Facility-based sampling |
Cross-sectional |
16.5% (220) of female sex workers reported having temporary marriage and 18.2% (40) of them had experiences HAS. |
7 |
| Repeated |
Khani et al, 2018
19
|
514 women referring to health care centers, Iran |
23-38 |
Multistage sampling |
Cross-sectional |
13 (2.6%) women had the experience of temporary marriage; (30%) of them experienced sexual coercion. |
7 |
| Repeated |
Dua’ Al-Maharma, et al,
2019.
38
|
523 Syrian refugee women, Jordan |
15-44 |
Proportional quota sampling |
Cross-sectional |
6.5% of women with temporary marriage experienced domestic violence and 9.1% of them suffered from sexual violence. |
7 |
|
Psychosocial disorders
|
| 27 |
Zarei et al, 2017
51
|
150 divorced women, Iran |
27-36 |
Convenience sampling |
Cross-sectional |
2.6% of divorced women reported having temporary marriage; the use of the Social Exclusion Questionnaire in Iranian divorced women indicates that women with temporary marriage had psychosocial effects. |
8 |
| 28 |
Salarifar, et al,
2015
52
|
60 householder women with temporary marriage and 60 householder women without temporary marriage, Iran |
28-38 |
Random sampling |
Case/Control |
The mean score of General Heath Questionnaire (GHQ)-test and Rif-test (Rehabilitation Psychological) indicated that the householder women with temporary marriage were better than householder women without temporary marriage indicating that the psychological and emotional state of women with temporary marriage is better. |
7 |
| 29 |
Ahmadi et al, 2011
53
|
1,025 Iranian soldiers, Iran |
|
Cluster sampling |
Cross-sectional |
2% of these soldiers reported having temporary marriage and tendency toward alcohol and multi-substance abuses. |
6 |
| Repeated |
PourReza et al, 2011
43
|
278 women with abortion, Iran |
15-49 |
Convenience sampling |
Cross-sectional |
33.4% of women with temporary marriage had an abortion and experienced psychological side effects. |
8 |
|
Other issues
|
30
|
Valizadeh et al, 2016
54
|
20 couples who were married without going to marriage center and without being screened for thalassemia, Iran |
16-30 |
Convenience sampling |
Cross-sectional |
25% of couples had temporary marriage and minor couple marriage. |
7 |
STIs: sexually transmitted infections; HIV: human immunodeficiency viruses; DIC: drop-in center; HAS: heterosexual anal sex; FSW: female sex workers ; HCVAb : hepatitis C virus antibody
Violence
Women with temporary marriage are at higher risk of violence and spousal abuse, compared to other women
47
. In the present review study, four studies were identified in this regard. The results of a study carried out by Eslamlou and Boshehri on women with spousal abuse referring to the Urmia Forensic Medicine Center, Iran, indicated that about 20% of the female complainants were women with temporary marriage. Domestic violence in females with temporary marriage was compared to that reported for women with permanent marriages (Adjusted OR: 4.6; CI 95%: 1.25-17.7; P=0.01). The authors suggested temporary marriage as the strongest risk factor for violence and spousal abuse
48
. Furthermore, a study conducted by Rahmani et al. demonstrated that 18.2% of women with temporary marriage had a lifetime experience of heterosexual anal sex
49
. The results of a study conducted by Merghati-Khoie et al. showed that addicted women with temporary marriage faced violence and all kinds of physical and sexual abuse, and condom use was positively associated with harassment and psychological abuse of women
50
. A study carried out by Khani and Moghadam in the north of Iran indicated that the main reason for these women’s referral to medical centers was sexual coercion and 85% of the participants in the aforementioned study also reported that their partners did not use a condom during intercourse. In fact, neglecting the health status and sanitary needs of women with temporary marriage is considered spousal abuse
19
. The Syrian young-female and older refugees in Jordan are sexually abused through a temporary marriage. About 6.5% of these refugees experienced spousal abuse and 9.1% of them had sexual abuse of any type, including coercion, forced intercourse, and anal sex during menstruation
38
.
Psychosocial disorders
Four studies were identified in this search with regard to psychosocial disorders. The results of a study carried out by Zarei et al. on divorced women with temporary marriage using the Social Exclusion Questionnaire in Iranian divorced women suggested that these women suffered from mental disorders, such as anxiety, depression, and psychosomatic disorders, due to a lack of social and economic support during and after the end of temporary marriage. Therefore, they have to look for a new relationship or an extension to their previous temporary marriage
51
. A study conducted by Pourreza and Batebi showed that 33.4% of women with temporary marriage had an abortion and experienced psychological side effects
44
. Another study performed by Salarifar demonstrated that the head of household with temporary marriage had a better mental, emotional, sexual, and physical status than the head of household without temporary marriage
52
. Moreover, Ahmadi et al. observed that temporary marriage was one of the predictive factors for drug abuse among young individuals
53
.
Other issues
In addition to the five above-mentioned topics, there are other issues. For example, the findings of a study carried out by Valizadeh et al. showed that out of 20 couples who got married without going to the marriage center and without being screened for thalassemia, 5 couples had temporary marriage and minor couple marriage
54
.
Discussion
In this systematic review, it was observed that STIs were very common in women with temporary marriage. The main causes of the increase in the prevalence of STIs among this population in different studies were the absence of trained health care and misjudgment by providers in reproductive and sexual health services, under-reporting, and poor notifications due to social stigma, causing them to be an important potential source of STIs, especially treatment-resistant STIs
28,55
. Furthermore, unprotected sex and lack of men’s participation in the use of barrier methods in sexual relations neglecting the health of women with temporary marriage and spousal abuse were other causes of the increase in the prevalence of STIs among this population
19,47
.
In sexual violence, victims are vulnerable to sexual and reproductive health consequences, such as unwanted pregnancies, unsafe abortions, and higher risk of STIs in unprotected sex
38
. Barriers to condom use seem to be socioculturally determined by gender stereotypes. In addition, stigma leads to a lack of control over the sources and culture of patriarchy in society, gender inequity, and lack of womenʼs negotiation power with men. These cause many problems, including less access to health care, economic dependency, and ultimately citizenship needs, among women with temporary marriage which are kinds of violence against women
32,56,57
. Spousal abuse or intimate partner violence as a health and social problem is accompanied by multiple physical and sexual, reproductive, and psychological health complications, poor quality of life, social consequences, and even mortality
47,34
.
On the other hand, one of the main reasons for abortion is temporary marriage. These marriages are not socially accepted and often remain secret from the couplesʼ families and community. This limits couples’ access to reproductive health services and may increase the risk of unintended pregnancy
40,58
. Temporary wives are forced to accept unsafe and illegal abortions due to a fear of stigmatization, prejudiced health care services, and absence of active services in sexual and reproductive health. Unsafe abortion is the third leading cause of maternal mortality and affects the physical, emotional, and social health of women and judicial
43
. Temporary marriage in countries in which it is prevalent is one of the strong predictors of unwanted pregnancy and unsafe abortion
40,59
due to the confirmation and proof of the father-child lineage, despite reliable experiments, is still difficult due to its high cost and lack of access
60
.
In addition, it is reported that some female adolescents who have not reached the legal age of marriage are forced to accept temporary marriage by their families or caregivers. The average rate of early marriage was reported as 16%, with 23% in Baluchestan as the highest rate in Iran
13
. When brides are much younger than their spouses, the gap in age will make them in a weaker position in case they need to express their physical, emotional, and health care needs that in turn cause more serious reproductive health complications, such as unwanted pregnancy, abortion, preterm labor, and fetal mortality
12,13
. In war-torn countries (e.g., Algeria, Sudan, Morocco, and Syria ), hundreds of women and girls have been sold under the guise of temporary marriage or girls are abducted or kidnapped by armed militia or rebels and forced into temporary marriage as a combination of child prostitution and pure slavery
10,61
. Syrian families in asylum countries have a disturbing sense of insecurity, vulnerability, and real and perceived risk of sexual harassment. Early marriage under the guise of protecting girls against poverty and insecure conditions saves their families from financial constraints
38,61
.
In several studies, it was indicated that women with temporary marriage mostly suffered from psychosocial issues causing two types of concerns including 1) intrapersonal communication disorders (e.g., anxiety, depression, and lack of self-esteem) and 2) interpersonal communication disorders (e.g., a lack of love and empathy)
61,62
. Numerous studies reported STIs, sexual abuse, unwanted pregnancy, and abortion as several possible outcomes of temporary marriage
63
. Finally, the existing stigma to temporary marriage has made this group extremely hard-to-access by the health care providers. It should be considered to address the sexual and reproductive health needs of women with temporary marriage. This paying attention to the sexual and reproductive health needs of this group of women not only protects their right to live longer and healthy lives but also is an important step toward maintaining the health of society. In fact, temporary marriage has made the vision of womenʼs rights and reproductive-sexual rights more complicated
19
.
Limitations
Throughout the world, most of the studies carried out on temporary marriage have been based on legal and jurisprudential approaches or qualitative studies; however, this topic with a health-oriented approach has been paid less attention. Culturally, the Middle East is a conservative society in which sexuality, sexual health issues, and temporary marriage are social taboos and women with temporary marriage due to a fear of stigmatization and social misjudgment avoid from undergoing medical care and are unaware of available or sufficient services
38
. Embarrassment would be one cause for concealing some relevant and important relationship information. For these reasons, studies conducted on women with temporary marriage with a health-oriented approach were under-reported and limited in number. Moreover, the use of nonrandom sampling restricted the generalizability of the findings and increased information bias and selection bias. Self-administered questionnaires provide a more private and less threatening means of reporting sensitive behaviors, thereby reducing information and reporting or recall bias or Sensitive study method can be used.
Conclusions
Temporary marriage is proposed as a legitimate sexual relationship between a man and a woman. However, the secrecy, lack of knowledge about the properties of temporary marriage among young girls or women, and lack of legal and organized social support for the temporary wives make this group socially, mentally, and physically vulnerable. Ignoring these concerns can put temporary wives at a higher risk of health, family, and social problems
50
. The absence of quality resources and services in reproductive and sexual health, under-reporting temporary marriage and its side effects, and lack of governmental and social support due to social stigma contribute to risky illegal and induced abortions, violence, early child marriage, and STIs among women with temporary marriage. Therefore, it is recommended to provide women with temporary marriage in legal age with legal and social supports, expand access to health education and sexual and reproductive services, and review womenʼs rights and reproductive-sexual health rights.
Acknowledgements
The present study was supported by Shahroud University of Medical Sciences as a PhD thesis (grant no.: 98119). Hereby, the authors would like to express their gratitude to the Research Deputy of Shahroud University of Medical Sciences.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The present study was supported by Shahroud University of Medical Sciences, Iran (code: 98119).
Highlights
-
Temporary marriage is a legitimate sexual relationship; however, it can be a threat to individuals and social health.
-
In this review, the potential effects of temporary marriage were sexually transmitted infections, unwanted pregnancies, abortions, violence, psychosocial disorders, and early marriage.
-
Wives with temporary marriage have an urgent need for sexual and reproductive health services in a safe and unprejudiced environment.
References
- Haeri S. Temporary marriage and the state in Iran: an Islamic discourse on female sexuality. Religion and Politics Journal 1992; 59(1):201-23. [ Google Scholar]
- Tremayne S. Change and ‘face’ in modern Iran. Journal of Anthropology Middle East 2011; 1(1):25-41. [ Google Scholar]
- Badran SZ, Turnbull B. Contemporary Temporary Marriage: A Blog-analysis of First-hand Experiences. International Women's Studies Journal 2019; 20(2):241-56. [ Google Scholar]
- Margalit Y. Temporary Marriage: A comparison of the Jewish and Islamic Conceptions. Journal of Law & Religion 2018; 33(1):89-95. [ Google Scholar]
- Aghajanian A, Vaezzade S, Kohan JA, Thompson V. Recent Trends of Marriage in Iran. Open Family Studies Journal 2018; 10(1):1-8. [ Google Scholar]
- El-Kak F. Sexuality and sexual health: constructs and expressions in the extended Middle East and North Africa. Vaccine 2013; 31:45-50. [ Google Scholar]
- DeJong J, Shepard B, Jawad R, Mortagy I. Young People’s Sexual and Reproductive Health in the Arab countries and Iran. Reprod Health Matters 2005; 13(25):49-59. [ Google Scholar]
- Abu-Raddad LJ, Hilmi N, Mumtaz G, Benkirane M, Akala FA, Riedner G. Epidemiology of HIV infection in the middle East and North Africa. AIDS 2010:24-38.
- Ghodsi T. Tying a slipknot: temporary marriages in Iran. Michigan Journal International Law 1994; 15(2):645-56. [ Google Scholar]
- Mikhail S. Child marriage and child prostitution: Two forms of sexual exploitation. In: Suzanne Williams RM, editor. Gender, Trafficking, and Slavery. Oxford UK: Published by Oxfam GB; 2002.
- Rashad H, Osman M, Roudi-Fahimi F. Marriage in the Arab world. Mishigan Arab World 2005; 24-35.
- Positives Y. Ending Child Marriage: A guide for global policy action. London: International Plan Parent Federation; 2010.
- Tremayne S. Modernity and early marriage in Iran: A view from within. Journal of Middle East Women’s Studies 2006; 2(1):65-94. [ Google Scholar]
- Shmuluvitz S, Witezman B. Temporary Marriage in Islam: Exploitative or Liberating?. Aviv Note 2012; 6(5):1-8. [ Google Scholar]
- Lo CKL, Mertz D, Loeb M. Newcastle-Ottawa Scale: Comparing reviewers’to authors’assessments. BMC Med Res Methodol 2014; 14(1):45. [ Google Scholar]
- Stang A. Critical Evaluation of the Newcastle-Ottawa scale for the assessment of the quality of non-randomized studies in meta-analyses. Eur J Epidemiol 2010; 25:603-5. [ Google Scholar]
- Luchini C, Stubbs B, Solmi M, Veronese N. Assessing the Quality of studies in Meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J Meta-Analysis 2017; 5(4):80-7. [ Google Scholar]
- Adib-Hajbaghery M, Zare M. The barriers to patient education from the viewpoint of nurses in Iran: A systematic review. Journal of Nurse and Midwifery Urmia University Medical Sciences 2017; 15(7):544-58. [ Google Scholar]
- Khani S, Moghadam B. Women’s sexual and reproductive health care needs assessment: an Iranian perspective. East Mediterr Heal 2018; 24(7):637-45. [ Google Scholar]
- Rostami F, Shokoohi M, Bamimore A M, Nasirian M, Asadi- Aliabadi M, Haghdoost A. Prevalence of sexually transmitted infections based on syndromic approach and associated factors among Iranian women. Iran J Heal Sci 2017; 5(1):1-12. [ Google Scholar]
- Shokoohi M, Karamouzian M, Mirzazadeh A, Haghdoost A, Rafierad A, Sedaghat A. HIV knowledge, attitudes, and practices of young people in Iran: Findings of a national population-based survey in 2013. PLoS One 2016; 11(9):23-34. [ Google Scholar]
- Kazem Mohammad, Farahani F. Sexual risk-taking behaviors among boys aged 15–18 years in Tehran. J Adolesc 2007; 41:407-14. [ Google Scholar]
- Hassani Azad M, Davoodian P, Boushehri E, Zade Saraji N. The Prevalence of Infection with the Human Immunodeficiency Virus (HIV) Among the Volunteers for Marriage Referred to the Health Center of Bandar Abbas in 2015. Techology Journal of Engineering and Applied Sciences 2016; 6(1):45-55. [ Google Scholar]
- Shokoohi M, Karamouzian M, Khajekazemi R, Osooli M, Sharifi H, Haghdoost AA. Correlates of HIV testing among female sex workers in Iran: Findings of a national bio-behavioural surveillance survey. PLoS One 2016; 11(1):42-52. [ Google Scholar]
- Rezaianzadeh A, Abbastabar H, Rajaeefard A, Hgaem H, Abdollahi M. Determinant factors of survival time in a cohort study on HIV patient using by time-varying cox model: Fars province, south of Iran. Int J Epidemiol Res 2017; 4(2):145-55. [ Google Scholar]
- Tehrani FR, Malek-Afzali H. Knowledge, attitudes and practices concerning HIV/AIDS among Iranian at-risk sub-populations. East Mediterr Heal J 2008; 14(1):142-56. [ Google Scholar]
- Nokhodian Z, Yazdani MR, Yaran M, Shoaei P, Mirian M, Ataei B. Prevalence and risk factors of HIV, syphilis, hepatitis B and C among female prisoners in Isfahan, Iran. Hepat Mon 2012; 12(7):92-7. [ Google Scholar]
- Fallahi A, Rahmani A, Azin SA, Molavi N, Higgs P, Allahqoli L. Effects of adverse early-life experiences on sexually transmitted infections among homelesswomen. Int J High Risk Behav Addict 2019; 8(3):43-53. [ Google Scholar]
- Kassaian N, Ataei B, Yaran M, Babak A, Shoaei P. Hepatitis B and C among women with illegal social behavior in Isfahan, Iran: Seroprevalence and associated factors. Hepat Mon 2011; 11(5):368-75. [ Google Scholar]
- Behzadi MA, Davarpanah MA, Namayandeh M, Pourabbas B, Allahyari S, Ziyaeyan M. Molecular diagnosis of genital tract infections among hiv-positive women in iran. Iran J Microbiol 2018; 10(4):233-41. [ Google Scholar]
- Zargooshi J. Characteristics of gonorrhoea in Kermanshah, Iran. Sex Transm Infect 2002; 78(6):460-71. [ Google Scholar]
- Shahesmaeili A, Karamouzian M, Shokoohi M, Kamali K, Fahimfar N, Nadji SA. Symptom-based versus laboratory-based diagnosis of five sexually transmitted infections in female sex workers in Iran. AIDS Behav 2018; 1(22):19-25. [ Google Scholar]
- Ghanbarzadeh N, Najafi A. Study of HIV and other sexually transmitted infections among female prisoners in Birjand. Journal of Birjand University Medical Sciences 2006; 13(328):69-74. [ Google Scholar]
- Asadi-Aliabadi M. High-risk behaviors among regular and casual female sex workers in Iran: a report from Western Asia. Iran J Psychiatry Behav Sci 2018; 4:54-61. [ Google Scholar]
- Merghti-Khoei ES, Rezaei Z, Shojaei-Zadeh Shojaei-Zadeh. Sexual Risk Behaviors and Condom Use Barriers in Iranian Men with Substance Use Disorders. Addict Heal 2017; 9(1):40-7. [ Google Scholar]
- Alipour A, Haghdoost AA, Sajadi L, Zolala F. HIV prevalence and related risk behaviours among female partners of male injecting drugs users in Iran: Results of a bio-behavioural survey, 2010. J Sex Trans Infect 2013; 89(3):41-7. [ Google Scholar]
- Shaditalab J, Azizzadeh B, Khanjaninejad L. The Need for Gender-Responsive Programs. United Nations Office for Drugs and Crime (UNODC). 2011.
- Al-Maharma D, Safadi R, Ahmad M, Halasa S, Nabolsi M, Dohrn J. Knowledge, attitudes and practices of Syrian refugee mothers towards sexually transmitted infections. Int J women Heal 2019; 19(11):607-15. [ Google Scholar]
- Essaid A, Usta J, Shukri S, El-Gharaibeh Y, Abu-Taleb H, Awwad N, et al. Gender based violence against women and girls displaced by the Syrian conflict in south Lebanon and North Jordan: scope of violence and health correlates. Lebanon: United Nations Population Fund (UNFPA); 2015.
- Cheraghi P, Poorolajal J, Moeini B, Cheraghi Z. Predictors of unintended pregnancy among married women in Hamadan, western Iran: A case-control study. Iran J Public Health 2013; 42(8):854-9. [ Google Scholar]
- Motaghi Z, Poorolajal J, Keramat A, Shariati M, Yunesian M, Masoumi SZ. Induced abortion rate in Iran: a meta-analysis. Arch Iran Med 2013; 16(10):594-8. [ Google Scholar]
- Francome C. Unsafe abortion and women’s health: Change and liberalization Unsafe Abortion and Women’s Health: Change and Liberalization. J Public Health 2016; 40(3):295-8. [ Google Scholar]
- Shahbazi S, Fathizadeh N, Taleghani F. Illegal abortions in Iran: a qualitative study. Journal of Advance Nursing 2009:1-9.
- Pourreza A, Batebi A. Psychological consequences of abortion among the post abortion care seeking women in Tehran. Iran J Psychiatry 2011; 6(1):31-6. [ Google Scholar]
- Jamshidi S, Saroukhani B. Study of unintended pregnancy and abortion rate in women who engage in temporary marriage. Fifth Iran International Conference Women’s Health; 18-19 May; Shiraz 2016.
- Jahanfar S, Sadat-Hashemi M, Ramazani F. Unwanted pregnancy in Tehran - What are the risk factors. International Journal of Gynecology and Obstirics 2000; 70:82-8. [ Google Scholar]
- Ghahari S, Khademolreza N. Spouse abuse in Iran: Where are we today?. Iranian Journal of Psychiatry and Clinical Psychology 2019; 24:458-62. [ Google Scholar]
- Eslamlou HR, Boshehri B. Investigating the spouse of harassment and some factors affecting it in those who refer to the legal medical center of Urmia city". Journal Urmia University Medical Sciences 2006; 18(3):554-62. [ Google Scholar]
-
Rahmani A, Mirzazadeh A, Allahqoli L, Sharifi H, Shokoohi M, Karamouzian M. The prevalence of and factors associated with heterosexual anal sex among Iranian female sex workers. Sexuality & Culture. 2020. 10.1007/s12119-020-09787-5
- Merghati-Khoei E, Rimaz S, Korte JE, Back SE, Brady KT, Abad M. Intimate partner violence and risky sexual behaviors among Iranian women with substance use disorders. Med J Islam Repub Iran 2015; 29(7):174-85. [ Google Scholar]
- Zarei F, Solhi M, Merghati-Khoei E, Taghdisi MH, Shojaeizadeh D, Taket AR. Development and psychometric properties of social exclusion questionnaire for Iranian divorced women. Iran J Public Heal 2017; 46(5):640-9. [ Google Scholar]
- Salarifar MR. Comparison of public health and optimal health of psychology, householder women with and without Temporary Marriage. Islam Psychology Studies Journal 2015; 8(15):67-86. [ Google Scholar]
- Ahmadi K, Mehrazmay A, Karambakhsh A, Salesi M. An investigation of demographic and familial characteristics of addicted soldiers. Journal of Military Medical 2013; 15(3):201-8. [ Google Scholar]
- Valizadeh F, Batebi AA, Pourreza A, Deylami A. Evaluation of the pregnant mother beta-thalassemia screening program. Journal School Public Health Institute of Public Health Research 2016; 14(2):39-50. [ Google Scholar]
- Asadi-AliAbadi M, Abolghasemi J, Rimaz S, Majdzadeh R, Rostami-Maskopaee F, Merghati-Khoei E. Barriers to health service utilization among Iranian female sex workers: a qualitative study. J Prev Med Public Heal 2018; 51(2):64-70. [ Google Scholar]
- Lotfi R, Tehrani FR, Yaghmaei F, Hajizadeh E. Barriers to condom use among women at risk of HIV/AIDS: A qualitative study from Iran. BMC Women's Health 2012; 12:32-41. [ Google Scholar]
- Lotfi R, Ramezani Tehrani F, Merghati Khoei E, Yaghmaei F, Dworkin SL. How do women at risk of HIV/AIDS in Iran perceive gender norms and gendered power relations in the context of safe sex negotiations?. Arch Sex Behav J 2013:873-81.
- Shamshri H. Knowledge and Attitudes of a Number of Iranian Policy-makers towards Abortion. J Reprod Infertil 2010; 11(3):189-95. [ Google Scholar]
- Motaghi Z, Keramat A, Shariati M, Yunesian M. Triangular assessment of the etiology of induced abortion in Iran: A qualitative study. Iran Red Cres Med J 2013; 15(11):92-8. [ Google Scholar]
- Ealami Gharebagh A TA. Proof of lineage in Iranian and Egyptian law. Jurisprud History Civiliz 2018; 5(53):117-56. [ Google Scholar]
- Khan MM, Khan H. Syrian crisis and its effects on medical community. Gomal J Med Sci 2016; 14(1):1-12. [ Google Scholar]
- Edalati A. A review: dominance, marital satisfaction and female aggression. Journal Social Sciences 2010; 6(2):162-8. [ Google Scholar]
- Kalantari AH, Fasaei S. A qualitative study on terms and conditions of women’s temporary marriage. Women Development Policies 2015; 12(4):507-24. [ Google Scholar]
- Merghati-Khoei E, Solhi M, Nedjat S, Taghdisi MH, Zadeh DS, Taket AR. How a Divorcee’s Sexual Life Is Socially Constructed and Understood in the Iranian Culture. Journal of Divorce Remarriage 2014; 55(5):335-47. [ Google Scholar]