J Res Health Sci. 21(3):e00524.
doi: 10.34172/jrhs.2021.56
Original Article
Evaluation of the Factors Affecting the Cure Rate of Cervical Intra-Epithelial Neoplasia Recurrence Using Defective Models
Nastaran Hajizadeh 1, Ahmad Reza Baghestani 2, *, Mohamad Amin Pourhoseingholi 3, Ali Akbar Khadem Maboudi 4, Farah Farzaneh 5, Nafiseh Faghih 5
Author information:
1Department of Biostatistics, Faculty of Paramedical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Physiotherapy Research Center, Department of Biostatistics, Faculty of Paramedical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Gastroenterology and Liver Diseases Research Center, Research Institute for Gastroenterology and Liver Diseases, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4Department of Biostatistics, Faculty of Paramedical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5Preventive Gynaecology Research Center, Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
*Correspondence: Ahmad Reza Baghestani (PhD) Tel: +98 21 22718531 Fax: +98 21 22721150 E-mail:
baghestani@sbmu.ac.ir
Abstract
Background: Treatment of cervical intraepithelial neoplasia is very important since if it remains untreated, it may progress to cervical cancer. It is usually treated with excisional surgery. This study aimed to find the factors affecting the cure rate of cervical intraepithelial neoplasia recurrence after surgery using defective models.
Study design: A retrospective cohort study.
Methods: Excisional surgery was performed on 307 patients with high-grade cervical intraepithelial neoplasia, from 2009 to 2017. The patients were followed up until recurrence based on histopathology report. Hematologic factors were measured before surgery. The cure rates were estimated using defective models with a Gamma frailty term and the results were compared.
Results: Neutrophil-to-lymphocyte ratio (NLR) (P<0.001) and excised mass size (P<0.001) had significant impacts on cure rates, and their cut-off values were 1.9 (P<0.001) and 15 mm2 (P<0.001), respectively. Patients with lower neutrophil-to-lymphocyte ratios and larger excised tissues had higher cure rates. Defective 3-parameter Gompertz distribution with gamma frailty term had the best fit to the data, and its estimated cure rates were 98% among patients with an excised mass size of >15 mm2 and NLR of <1.9, 84% among patients with an excised mass size of >15 mm2 and NLR of >1.9, 79% among patients with an excised mass size of <15 mm2 and NLR of <1.9, and 30% among patients with an excised mass size of <15 mm2 and NLR of >1.9.
Conclusion: Cervical intraepithelial neoplasia must be identified and treated before its progress. Excision of more tissues during excisional surgery, especially when the NLR of the patient is high, can help to prevent cervical intraepithelial neoplasia recurrence.
Keywords: Cervical intra-epithelial neoplasia, Cure rate, Defective models, Survival analysis
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Citation: Hajizadeh N, Baghestani AR, Pourhoseingholi MA, Khadem Maboudi AA, Farzaneh F, Faghih N. Evaluation of the Factors Affecting the Cure Rate of Cervical Intra-Epithelial Neoplasia Recurrence Using Defective Models. J Res Health Sci. 2021; 21(3): e00524.
Introduction
Cervical cancer is the third most frequent cancer among women, with an age-standardized incidence rate of 13.1 per 100,000 and an age-standardized mortality rate of 6.9 per 100,000 in the world
1
. The pre-invasive cervical lesion is a type of detectable epithelial change which if left untreated, may progress to an advanced form of cervical cancer
2
. Therefore, detection and treatment of cervical intraepithelial neoplasia (CIN) as a pre-invasive lesion can prevent cervical cancer
3-7
.
Generally, CIN is divided into three grades: (i) CIN I which is equivalent to mild dysplasia, (ii) CIN II which is equivalent to moderate dysplasia, and (iii) CIN III which is equivalent to severe dysplasia or in-situ carcinoma and recognized as a true pre-invasive precursor with a potential to progress to cancer
8,9
. The CIN II and III are often treated with one of the local excisional procedures which has proved to be effective
10
. The most common CIN excisional procedures are large loop excision of the transformation zone, loop electrosurgical excision procedure, laser conization, and cold-knife conization
11,12
.
There are several factors that could play significant roles in the prediction of CIN recurrence rate, such as age, marginal involvement of the sample, glandular involvement, chronic inflammation caused by bacterial or viral infections, and the status of the immune system of the body
13-15
. There are various factors for checking the status of the immune system. Among them, neutrophil–to–lymphocyte ratio (NLR) is an effective marker of inflammation and is calculated by dividing the absolute peripheral blood neutrophils count by the absolute lymphocytes count
16
.
Standard survival models assume that all subjects are susceptible to the event of interest (such as recurrence or death from the disease)
17,18
. However, in practice, some individuals will never experience the event of interest; these risk-free subjects are called ‘‘cured’’. Existence of the cured fraction is indicated by a long flat tail which is not close to zero in Kaplan-Meier curves
19
as it is shown in Figure 1.
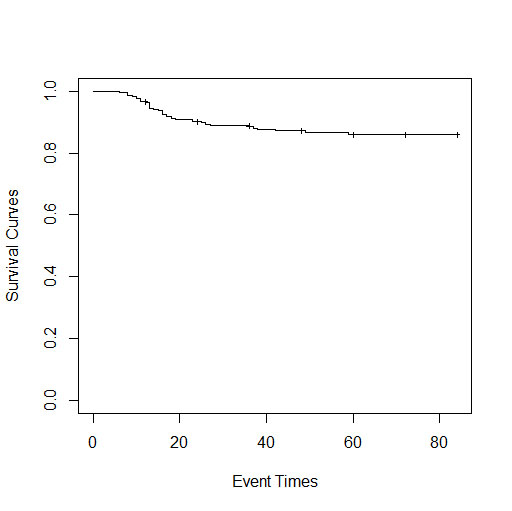
Figure 1.
Kaplan-Meier curve of the cervical intraepithelial neoplastic data
.
Kaplan-Meier curve of the cervical intraepithelial neoplastic data
The mixture models are usually used for cure rate modeling. The survival function of the standard mixture model is S(t)=p+(1-p)S0(t), where p∈(0,1) and S0(t) is a usual survival function that converges to zero as time goes to infinity. Therefore, S(t) converges to p with the passage of time
17
. Recently, defective distributions are used for cure rate modeling
20
. Defective distributions have the ability to become a cure rate model by changing the usual domain of its parameters without adding any extra parameters to the model. It should be mentioned that the parameters whose domains change are called defective parameters
20
. The proportion of the cured population is acquired by calculating the limit of the defective survival function which is a value between zero and one
21-25
. There are two defective distributions in the related literature, namely the Gompertz and the Inverse Gaussian distributions.
It is known that two subjects with the same observed characteristics may have different survival times due to the factors that are not or could not be observed among people, such as genetic and environmental factors. Frailty models accommodate the unobserved heterogeneity by the inclusion of a random effect in the model which is called an individual frailty term and improves the fit of the model. The gamma distribution is commonly used for the frailty term
26
.
The present study aimed to estimate the cured fraction and identify the factors affecting the cure rate of CIN recurrence among 307 women treated with CIN excisional surgery using defective models with frailty terms.
Methods
The required data were collected from a historical cohort study performed on 307 patients with CIN-positive pathology. They had excisional treatment at the Department of Oncology, Imam Hossein Hospital, Tehran, Iran from 2009 to 2017 and were followed up until January 2018
27
. It should be mentioned that during this period, 514 individuals were treated, while 14 of them were excluded due to impairment of immunity and underlying illnesses, and 193 of them were excluded due to the lack of follow-up. During this period, individuals with high-grade CIN (II and III) were treated by loop electrosurgical excision procedure or cold-knife conization excisional procedures and were followed up with performing colposcopy at 6 and 12 months, and then annually.
The recurrence was determined by histopathology report, and the time interval between surgery and recurrence was considered the survival time. The survival time is right-censored for patients without recurrence. Also, in the case of hysterectomy, the patients were usually cured, therefore, their survival time was considered as right-censored. Demographic, clinical, pathological, and hematological findings of these patients were extracted from their records. Moreover, complete blood count tests were taken before surgery and the NLR and platelet–to–lymphocyte ratio indexes were calculated using neutrophil, platelet, and lymphocyte counts reported in the blood test.
Regarding ethical considerations, written informed consent was obtained from patients and the study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (IR.SBMU.RETECH. 1397.1360).
Statistical analysis
Mean and standard deviation values were presented for quantitative variables and evaluated based on one-way ANOVA test. Frequency and percentage were presented for qualitative variables and evaluated using the Chi-square test. Effects of different variables on the cure rate were assessed using two defective models with a frailty term: the defective Gompertz model with Gamma frailty term (defective Gamma Gompertz model), and the defective 3-parameter Gompertz model with Gamma frailty term (defective Gamma 3-parameter Gompertz model)
28,29
. It should be mentioned that the inverse Gaussian model with gamma frailty term was also fitted to the data but was not able to estimate the cure rate in this dataset. This is why this model is not explained here.
The survival function of the Gompertz distribution with gamma frailty term is as follows:
Here, α>0 represents the shape parameter, θ>0 is the frailty term, and xTβ=b0+b1x1+b2x2+…bkxk in which β=(b0,b1,…, bk) indicates the coefficients vector andxT=(1,x1, x2,…, xk) indicates the covariates vector. When α<0, we have the defective gamma-Gompertz (DGG) model and θ∈R.
The hazard function of the DGG model is as follows:
(2)
The cure fraction of the DGG model is calculated based on the following formula:
(3)
The survival function of the 3- parameter Gompertz distribution with gamma frailty term is as follows:
(4)
Here, α and η are shape parameters and belong to real values, θ>0 is the frailty term, and xTβ=b0+b1x1+b2x2+…bkxk in which β=(b0,b1,…, bk) indicates the coefficients vector and xT=(1,x1, x2,…, xk) indicates the covariates vector. When α<0, we have the defective gamma 3-parameter Gompertz (DGG3) model and θ∈R.
The hazard function of the DGG3 model is as follows:
(5)
The cure fraction of the DGG3 model is calculated based on the following formula:
(6)
The backward selection method was used to find more useful predictors among all the predictors in the models. The backward selection is a method of fitting models with all candidate variables and testing the deletion of each variable using a chosen model fit criterion. In this method, the variable whose loss leads to the most insignificant deterioration of the model fit is deleted and this process is repeated until no further variables can be deleted from the model without any significant loss of fit. Selection aims to reduce the set of predictor variables to those that are necessary and account for nearly as much of the variance as is accounted for by the total set
30
. The best model was selected based on Akaike Information Criteria (AIC) and by comparison of the fitted survival curves with the Kaplan-Meier curves. The lower the AIC and the closer the fitted curves to the Kaplan-Meier curves, the better the model.
For better interpretability of the results, cut-off values were considered for the selected predictors. Two methods were used to find the cut-off values. The first method was using a receiver operating characteristics curve (ROC) and calculating the Youden index. The Youden index is calculated based on the following formula: J=sensitivity+specificity-1. In this formula, sensitivity is the ability of a test to correctly identify patients with recurrence, and specificity is the ability of a test to correctly identify people without recurrence. The Youden index value ranges from zero to one, and a value of one indicates that the test is perfect. The index is calculated for all points of a ROC curve, and the maximum value of the index is used as a criterion for selecting the optimum cut-off point. This method only considers the recurrence status
31,32
.
The second method was using the log-rank test which considers the survival times in addition to the recurrence status of the patients. It is a nonparametric test and is appropriate for usage in survival analysis
33
. Parameters of the models were estimated using the maximum likelihood estimation method. Maximum likelihood estimation is a method of estimating the parameters of a probability distribution by maximizing the likelihood function in a way that the observed data is most probable under the assumed statistical model. For this purpose, a code was written in R software (version 3.2.1) and the Broyden–Fletcher–Goldfarb–Shanno maximization method in the Optim package was used
34
. The codes are available upon request.
Results
Table 1 summarizes the demographic and clinical information of 307 patients treated with CIN excisional surgery. The median and mean values of the survival time of patients were 60 and 75.17 months, respectively (95% CI: 72.54, 77.80). Moreover, the minimum and maximum follow-up times were 12 and 84 months, respectively. It is also noteworthy that recurrence was observed in 38 (12.4%) patients. The model containing the excised mass size and NLR variables had the lowest AIC among the fitted models; therefore, these two variables were selected to predict the cure rates among patients.
The area under the ROC curve (AUC) was remarkable for the diagnosis of recurrence based on the excised mass size predictor (AUC=0.852; 95% CI: 0.789, 0.916; P<0.001). The cut-off point of the excised mass size was obtained at 15 mm2 using the Youden index. The sensitivity and specificity values of the excised mass size cut-off point in the diagnosis of recurrence were 0.874; (95% CI: 0.678, 0.905) and 0.732; (95% CI: 0.653, 0.789), respectively (Figure 2.a). Furthermore, a cutting point of 15 mm2 was found for the excised mass size using the log-rank test (P<0.001). The AUC of the ROC curve for the diagnosis of recurrence based on the NLR predictor was remarkable (AUC=0.801; 95% CI: 0.723, 0.879; P<0.001).
The NLR cut-off point of 1.9 was obtained using the Youden index. The sensitivity and specificity values of the NLR cut-off point in the diagnosis of recurrence were 0.737 (95% CI: 0.569, 0.866) and 0.739 (95% CI: 0.682, 0.79), respectively (Figure 2.b). In addition, a cutting point of 1.9 was found for NLR using the log-rank test (P<0.001). The excised mass size was <15 mm2 in 58 (18.9%) patients and ≥15 mm2 in 249 (81.1%) patients. The recurrence rates in patients with low and high excised mass sizes were 41.4% and 5.6%, respectively. The NLR was <1.9 in 209 (68.1%) and ≥1.9 in 98 (31.9%) patients. The recurrence rates in patients with NLR of <1.9 and >1.9 were 4.8% and 28.6%, respectively.
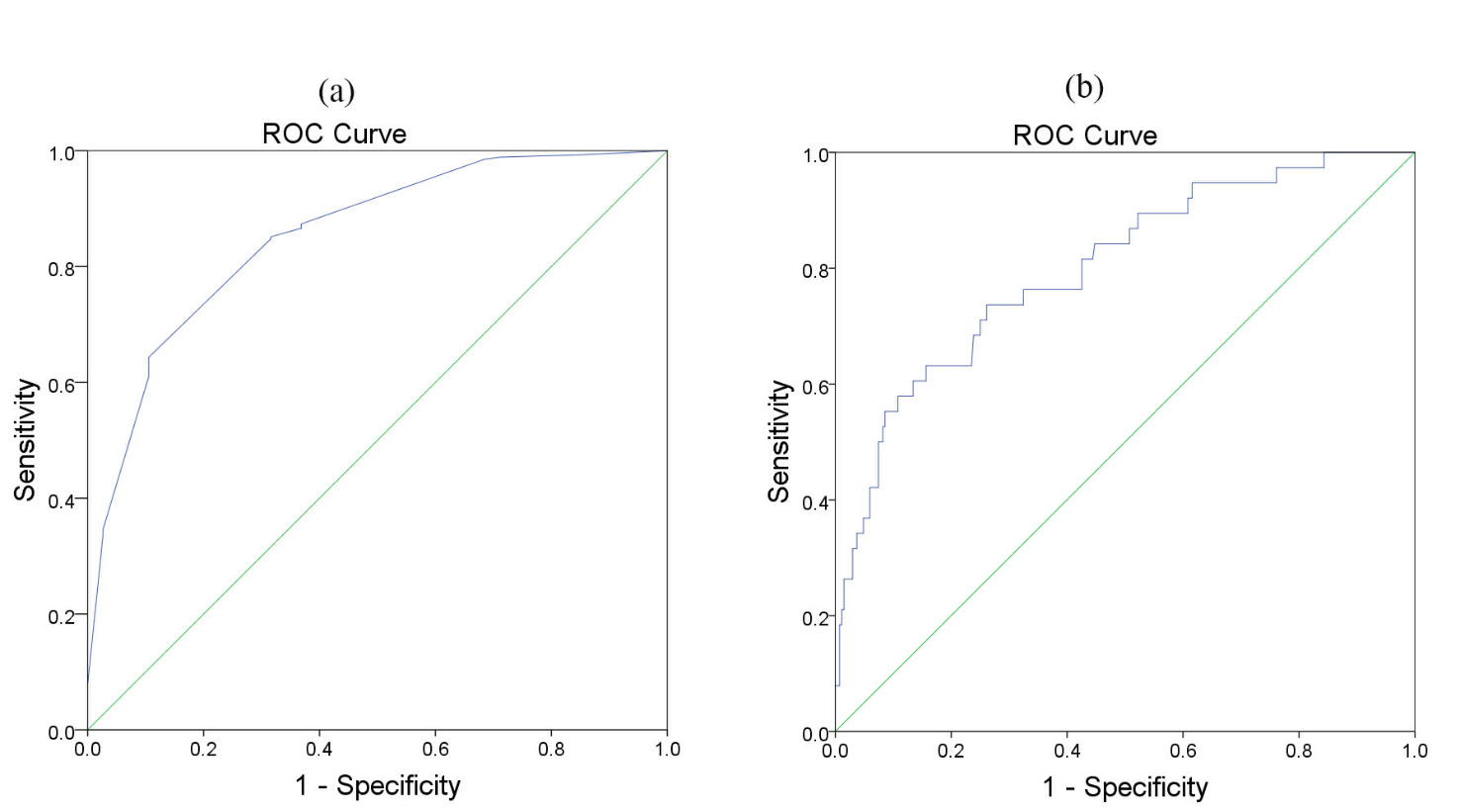
Figure 2.
Receiver operating characteristics curves of (a) excised mass size, and (b) neutrophil-to-lymphocyte ratio for predicting recurrence
.
Receiver operating characteristics curves of (a) excised mass size, and (b) neutrophil-to-lymphocyte ratio for predicting recurrence
Estimated values of the parameters of the DGG model are (α, θ, b0, b1, b2) = (-2.36, -0.51, -0.53, -1.92, 1.56) with standard errors of 0.23, 0.97, 0.26, 0.11, and 0.07 respectively. In the parameters vector, b0, b1, and b2 are the intercept, the coefficient of the excised mass size variable (P<0.001), and the coefficient of the NLR variable (P<0.001), respectively. The estimated values are substituted in formula 3 and the cure fractions are calculated for different categories of the covariates. It must be noted that the covariates x1=excised mass size and x2=NLR are considered as discrete and take zeros and ones for values lower and greater than the cut-off point values, respectively.
Table 1.
Description and comparison of the demographic and hematologic factors of patients based on the NLR and the excised mass size levels
|
Variables
|
Total (n=307)
|
NLR<1.9 and
mass size>15
(n=175)
|
NLR>1.9 and
mass size>15
(n=74)
|
NLR<1.9 and
mass size<15
(n=33)
|
NLR>1.9 and
mass size<15
(n=25)
|
P-
value
|
|
Continuous
|
Mean
|
SD
|
Mean
|
SD
|
Mean
|
SD
|
Mean
|
SD
|
Mean
|
SD
|
| Age |
40.36 |
9.14 |
40.57 |
9.59 |
40.62 |
8.43 |
40.76 |
8.54 |
37.6 |
8.70 |
0.479 |
| Parity |
2.74 |
1.91 |
2.79 |
1.09 |
2.61 |
1.94 |
2.94 |
1.69 |
2.522 |
1.53 |
0.758 |
| MCV |
84.71 |
8.50 |
84.92 |
7.62 |
84.63 |
7.61 |
83.64 |
14.65 |
84.81 |
5.98 |
0.888 |
| HB |
12.317 |
1.19 |
12.22 |
1.09 |
12.55 |
1.19 |
12.75 |
1.24 |
11.68 |
1.44 |
0.069 |
| RBC |
4.37 |
0.47 |
4.33 |
0.40 |
4.49 |
0.48 |
4.34 |
0.59 |
4.34 |
0.41 |
0.863 |
| WBC |
7263.84 |
1842.69 |
7106.29 |
1695.67 |
7224.32 |
1637.56 |
7096.97 |
1669.29 |
7304.00 |
1861.88 |
0.061 |
| PLT |
259.74 |
64.66 |
262.02 |
61.47 |
256.08 |
73.89 |
256.75 |
62.47 |
258.52 |
63.31 |
0.912 |
| PLR |
113.27 |
46.10 |
108.86 |
37.41 |
120.74 |
50.90 |
102.96 |
30.76 |
115.76 |
64.55 |
0.061 |
|
Categorical
|
Number
|
Percent
|
Number
|
Percent
|
Number
|
Percent
|
Number
|
Percent
|
Number
|
Percent
|
P-
value
|
| Delivery Type |
|
|
|
|
|
|
|
|
|
|
0.098 |
| NVD |
228 |
74.3 |
130 |
74.3 |
53 |
71.6 |
25 |
75.8 |
20 |
80 |
|
| CS |
60 |
19.2 |
39 |
22.3 |
11 |
14.9 |
6 |
18.2 |
4 |
16 |
|
| None |
19 |
6.5 |
6 |
3.4 |
10 |
13.5 |
2 |
6.1 |
1 |
4 |
|
| Cigarette |
|
|
|
|
|
|
|
|
|
|
0.542 |
| Yes |
10 |
3.3 |
5 |
2.9 |
4 |
5.4 |
0 |
0 |
1 |
4 |
|
| No |
297 |
96.7 |
170 |
97.1 |
70 |
94.6 |
33 |
100 |
24 |
96 |
|
| Treatment type |
|
|
|
|
|
|
|
|
|
|
0.148 |
| LEEP |
236 |
76.9 |
128 |
73.1 |
60 |
81.1 |
25 |
75.8 |
23 |
92 |
|
| Conization |
71 |
23.1 |
47 |
26.9 |
14 |
18.9 |
8 |
24.2 |
2 |
8 |
|
| Human Papilloma Virus |
|
|
|
|
|
|
|
|
|
|
0.359 |
| Positive |
35 |
11.4 |
24 |
13.7 |
7 |
9.5 |
1 |
3 |
3 |
12 |
|
| Negative |
9 |
2.9 |
5 |
2.9 |
1 |
1.4 |
1 |
3 |
2 |
8 |
|
| Unknown |
263 |
85.7 |
146 |
83.4 |
66 |
89.2 |
31 |
93.9 |
20 |
80 |
|
| Margin |
|
|
|
|
|
|
|
|
|
|
0.059 |
| Involved |
28 |
9.1 |
14 |
6.9 |
7 |
10.8 |
3 |
6.1 |
4 |
24 |
|
| Uninvolved |
279 |
90.9 |
163 |
93.1 |
66 |
89.2 |
31 |
93.9 |
19 |
76 |
|
| Treatment cause |
|
|
|
|
|
|
|
|
|
|
0.597 |
| CIN I |
46 |
14.9 |
22 |
12.6 |
14 |
19.6 |
6 |
17.2 |
4 |
15.4 |
|
| CIN II |
204 |
66.5 |
117 |
67.2 |
47 |
65.2 |
25 |
71.4 |
15 |
57.7 |
|
| CIN III |
57 |
18.6 |
35 |
20.2 |
11 |
15.2 |
4 |
11.4 |
7 |
25.9 |
|
NLR: neutrophil-to-lymphocyte ratio, MCV: mean corpuscular volume, Hb: hemoglobin concentration, RBC: Red blood cell count, WBC: white blood cell count, PLT: platelet, PLR: platelet-to-lymphocyte ratio, NVD: natural vaginal delivery, CS: cesarean section, LEEP: Loop Electrosurgical Excision Procedure, CIN: cervical intraepithelial neoplasia
Figure 3.a shows the comparison of the Kaplan-Meier curves with the curves of the fitted DGG model. The cure fractions of patients with the excised mass size of >15 mm2 and NLRs of <1.9 and >1.9 were estimated at 96% and 83%, respectively. Furthermore, cure fractions of patients with the excised mass size of < 15 mm2 and NLRs of <1.9 and >1.9 were estimated to be 76% and 16%, respectively.
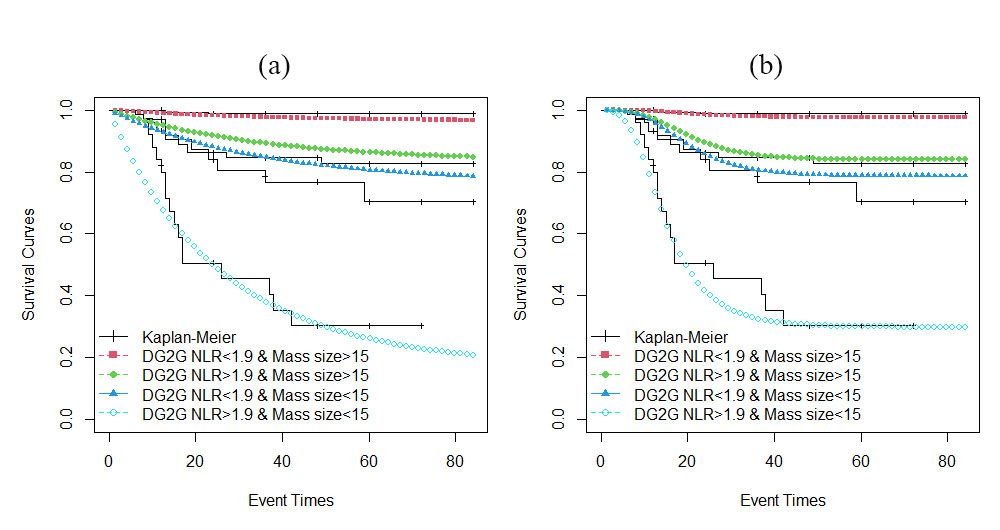
Figure 3.
Comparison of the Kaplan-Meier curves with (a) defective gamma Gompertz and (b) defective gamma 3-parameters Gompertz models
.
Comparison of the Kaplan-Meier curves with (a) defective gamma Gompertz and (b) defective gamma 3-parameters Gompertz models
Estimated values of the parameters of the DGG3 model are (α,θ,η,b0, b1,b2)=(-9.71, 0.82,-7.58, 2.97, -2.39, 2.05) with standard errors of 0.16, 0.42, 0.37, 0.05, 0.09, and 0.11, respectively. In the parameters vector, b0, b1, and b2 are the intercept, coefficient of the excised mass size variable (P<0.001), and coefficient of the NLR variable (P<0.001), respectively. The estimated values are substituted in formula 6 and the cure fractions are calculated for different categories of the covariates. As described above, the covariates are considered discrete. Figure 3.b shows the comparison of the Kaplan-Meier curves with the curves of the fitted DGG3 model.
The cure fraction among patients with the excised mass size of >15 mm2 and NLR <1.9 is estimated to be 98%, among patients with excised mass size >15 mm2 and NLR>1.9 is estimated to be 84%, among patients with excised mass size<15 mm2 and NLR<1.9 is estimated to be 79%, and among patients with excised mass size<15 mm2 and NLR>1.9 is estimated to be 30%.
The AICs of the DGG and DGG3 models are 123.1 and 105.3, respectively. Furthermore, according to Figure 3, the estimated curves of the DGG3 model were flattened close to Kaplan-Meier curves, while the curves of the DGG model are still decreasing. Hence, it can be said that the DGG3 model provides a better fit to the data.
Based on the survival curves of the DGG3 model (Figure 3.b) which was the best model based on AIC criteria, it can be said that patients with the excised mass size of >15 mm2 and NLR <1.9 are cured provided that they do not experience recurrence until 31 months after the treatment. Moreover, patients with the excised mass size of >15 mm2 and NLR of >1.9 are cured provided that they do not experience recurrence until 55 months after the treatment. In addition, patients with the excised mass size of <15 mm2 and NLR of <1.9 are cured provided that they do not experience recurrence until 52 months after the treatment. Finally, patients with the excised mass size of <15 mm2 and NLR of >1.9 are cured provided that they do not experience the recurrence until 59 months after the treatment. These time limits are based on the time (horizontal axis) where the fitted survival curves reach a plateau.
Discussion
In this study, it was found that the lower levels of NLR before surgery and an increase in the excised mass size lead to an increase in the cure rate from CIN recurrence among patients who underwent an excisional procedure for CIN. Cure rate models are important methods for the analysis of time-to-event data when there are risk-free individuals. It was common to use mixture models for cure rate modeling; however, recently, defective models are used for the analysis of data with cure fraction.
Defective models have the advantage of allowing a cure rate without requiring any extra parameters in the model and the proportion of the cured people is obtained by calculating the limit of the survival function and substituting the estimated parameters
28
. Moreover, the results of a study that compared the defective models with the mixtures model have indicated that the defective models fit better than the mixture models
28
. Presence of a frailty term in the model accounts for the unobserved heterogeneity and improves the fit of the model. The DGG3 model had a better fit on the data in comparison with the DGG model. Despite the existence of cured people in this dataset, the inverse Gaussian distribution could not estimate the cure fraction.
It was found that patients with lower NLR levels have more cure rates from CIN recurrence. Several studies on the effect of NLR, as a prognostic factor, on different cancers, such as colorectal, lung, and cervical cancers, revealed that patients with higher NLR levels prior to surgery had a shorter disease-free survival
27,35-37
. Misunuma et al.
38
and Chun et al.
39
also investigated the relationship between NLR and recurrence-free survival after the excisional procedure for the treatment of CIN. They found the same results but suggested a cut-off value of 2.1 for the NLR with sensitivity and specificity values of 0.571 and 0.745, respectively. The cut-off value of 1.9 for NLR found in this study had more sensitivity and specificity than that used by Chun et al.
39
.
It was found that the size of the excised tissue during excisional surgery had a direct relationship with the cure rate. Results of a similar study showed that a one-centimeter increase in the excised mass size reduced the hazard of recurrence by 68%. In the aforementioned study, it was also declared that due to the multifocal nature of CIN, removing larger tissues during surgery is accompanied by skip lesion and can decrease the chance of recurrence
40
. Nevertheless, the side effects, such as pregnancy-related complications, should be considered and a balance should be maintained between the two.
Conclusions
To prevent cancer and infertility, CIN patients must be identified and treated before the disease progresses and becomes invasive. Based on the findings, the NLR and excised mass size were the strongest predictive factors of the CIN recurrence. Removal of larger tissues during surgery, especially among patients with high NLR levels before the operation, can decrease the chance of recurrence after treatment. It should also be noted that using appropriate cure rate models is very important when there is a cure fraction in the data, otherwise, it may lead to incorrect estimates of the cure rates.
Acknowledgments
The authors would like to thank the reviewers and the editors for their comments which greatly improved this paper.
Conflict of interests
The authors declare that there are no conflicts of interest in this study.
Funding
This research is not financially supported.
Highlights
-
Neutrophil–to–lymphocyte ratio before surgery and excised mass size had significant impacts on cure rates among cervical intraepithelial neoplasia patients.
-
Patients with a neutrophil–to–lymphocyte ratio of lower than 1.9 had a higher chance of getting cured.
-
Patients with an excised mass larger than 15 mm2 had a higher chance of getting cured.
-
An increase in excised mass size during surgery has a direct relationship with the cure rate especially among patients with a high neutrophil–to–lymphocyte ratio.
-
When there is a cured fraction in data, it is important to use suitable cure models for the achievement of reliable results. Defective models are good choices for flexibly modeling the cure rate.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68(6):394-424. [ Google Scholar]
- Garcia F, Hatch KD, Berek JS. Intraepithelial Disease of the Cervix, Vagina, and Vulva. 15th ed. Berek and Novak’s Gynecology. Berek JS, editor, Philadelphia: Lippincott Williams and Wilkins 2012; p: 574-618.
- IARC. IARC handbooks of cancer prevention: cervix cancer screening. Vol 10. IARC Press. 2005.
- Landy R, Pesola F, Castañón A, Sasieni P. Impact of cervical screening on cervical cancer mortality: estimation using stage-specific results from a nested case–control study. Br J Cancer 2016; 115(9):1140-6. [ Google Scholar]
- Chen JY, Wang ZL, Wang ZY, Yang XS. The risk factors of residual lesions and recurrence of the high-grade cervical intraepithelial lesions (HSIL) patients with positive-margin after conization. Medicine (Baltimore) 2018; 97(41):e12792. [ Google Scholar]
- McCredie MR, Sharples KJ, Paul C, Baranyai J, Medley G, Jones RW. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: a retrospective cohort study. Lancet Oncol 2008; 9(5):425-34. [ Google Scholar]
- Kyrgiou M, Valasoulis G, Founta C, Koliopoulos G, Karakitsos P, Nasioutziki M. Clinical management of HPV‐related disease of the lower genital tract. Ann N Y Acad Sci 2010; 1205:57-68. [ Google Scholar]
- Tainio K, Athanasiou A, Tikkinen KA, Aaltonen R, Cárdenas J, Glazer-Livson S. Clinical course of untreated cervical intraepithelial neoplasia grade 2 under active surveillance: systematic review and meta-analysis. BMJ 2018; 27:360-499. [ Google Scholar]
- Rock JA, Jones III HW. Cervical cancer precursors and their management. TeLinde’s Operative Gynaecology, 9th Ed. Lippincort Williams & Wilkins; 2003.
- Kalliala I, Anttila A, Pukkala E, Nieminen P. Risk of cervical and other cancers after treatment of cervical intraepithelial neoplasia: retrospective cohort study. BMJ 2005; 331(7526):1183-5. [ Google Scholar]
- Martin-Hirsch PL, Paraskevaidis E, Kitchener H. Surgery for cervical intraepithelial neoplasia. Cochrane Database Syst Rev 2013(12):CD001318.
- Arbyn M, Redman CW, Verdoodt F, Kyrgiou M, Tzafetas M, Ghaem-Maghami S. Incomplete excision of cervical precancer as a predictor of treatment failure: a systematic review and meta-analysis. Lancet Oncol 2017; 18(12):1665-79. [ Google Scholar]
- Lodi CT, Michelin MA, Lima MI, Teixeira NC, Adad SJ, Murta EF. Factors associated with recurrence of cervical intraepithelial neoplasia after conization in HIV-infected and noninfected women. Arch Gynecol Obstet 2011; 284(1):191-7. [ Google Scholar]
- Lili E, Chatzistamatiou K, Kalpaktsidou-Vakiani A, Moysiadis T, Agorastos T. Low recurrence rate of high-grade cervical intraepithelial neoplasia after successful excision and routine colposcopy during follow-up. Medicine (Baltimore) 2018; 97(4):e9719. [ Google Scholar]
- Del Mistro A, Matteucci M, Insacco EA, Onnis G, Da Re F, Baboci L. Long-term clinical outcome after treatment for high-grade cervical lesions: a retrospective monoinstitutional cohort study. Biomed Res Int 2015; 2015:984528. [ Google Scholar]
- Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil–lymphocyte ratio: experience in patients with cancer. Critic Rev Oncol Hematol 2013; 88(1):218-30. [ Google Scholar]
- Masud A, Tu W, Yu Z. Variable selection for mixture and promotion time cure rate models. Stat Methods Med Res 2018; 27(7):2185-99. [ Google Scholar]
- Cox DR. Regression models and life‐tables. J R Stat Soc Series B Stat Methodol 1972; 34(2):187-202. [ Google Scholar]
- Sy JP, Taylor JM. Estimation in a Cox proportional hazards cure model. Biometrics 2000; 56(1):227-36. [ Google Scholar]
- Balka J, Desmond AF, McNicholas PD. Review and implementation of cure models based on first hitting times for Wiener processes. Lifetime Data Anal 2009; 15(2):147-76. [ Google Scholar]
- Haybittle JL. The estimation of the proportion of patients cured after treatment for cancer of the breast. British J Radiol 1959; 32(383):725-33. [ Google Scholar]
- Cantor AB, Shuster JJ. Parametric versus non‐parametric methods for estimating cure rates based on censored survival data. Stat Med 1992; 11(7):931-7. [ Google Scholar]
- Gieser PW, Chang MN, Rao PV, Shuster JJ, Pullen J. Modelling cure rates using the Gompertz model with covariate information. Stat Med 1998; 17(8):831-9. [ Google Scholar]
- Balka J, Desmond AF, McNicholas PD. Bayesian and likelihood inference for cure rates based on defective inverse Gaussian regression models. J Appl Stat 2011; 38(1):127-44. [ Google Scholar]
- Whttmore GA. An inverse Gaussian model for labour turnover. J R Stat Soc Ser A 1979; 142(4):468-78. [ Google Scholar]
- Vaupel JW, Manton KG, Stallard E. The impact of heterogeneity in individual frailty on the dynamics of mortality. Demography 1979; 16(3):439-54. [ Google Scholar]
- Farzaneh F, Faghih N, Hosseini MS, Arab M, Ashrafganjoei T, Bahman A. Evaluation of neutrophil–Lymphocyte ratio as a prognostic factor in cervical intraepithelial neoplasia recurrence. Asian Pac J Cancer Prev 2019; 20(8):2365. [ Google Scholar]
- Scudilio J, Calsavara VF, Rocha R, Louzada F, Tomazella V, Rodrigues AS. Defective models induced by gamma frailty term for survival data with cured fraction. J Appl Stat 2019; 46(3):484-507. [ Google Scholar]
- Haile SR, Jeong JH, Chen X, Cheng Y. A 3-parameter Gompertz distribution for survival data with competing risks, with an application to breast cancer data. J Appl Stat 2016; 43(12):2239-53. [ Google Scholar]
- Frank E. Harrell Jr. Regression modeling strategies. Springer; 2003.
- Youden WJ. Index for rating diagnostic tests. Cancer 1950; 3(1):32-5. [ Google Scholar]
- Schisterman EF, Perkins NJ, Liu A, Bondell H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005; 16(1):73-81. [ Google Scholar]
- Baghestani AR, Moghaddam SS, Majd HA, Akbari ME, Nafissi N, Gohari K. Survival analysis of patients with breast cancer using weibull parametric model. Asian Pac J Cancer Prev 2016; 16(18):8567-71. [ Google Scholar]
-
GBIF Secretariat. R Core Team, R: A Language and Environment for Statistical Computing. (Cited 20 May 2021). Available from: https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing.
- Walsh SR, Cook EJ, Goulder F, Justin TA, Keeling NJ. Neutrophil‐lymphocyte ratio as a prognostic factor in colorectal cancer. J Surg Oncol 2005; 91(3):181-4. [ Google Scholar]
- Sarraf KM, Belcher E, Raevsky E, Nicholson AG, Goldstraw P, Lim E. Neutrophil/lymphocyte ratio and its association with survival after complete resection in non–small cell lung cancer. The J Thorac Cardiovasc Surg 2009; 137(2):425-8. [ Google Scholar]
- Muriana P, Carretta A, Ciriaco P, Bandiera A, Negri G. Assessment of the prognostic role of neutrophil-to-lymphocyte ratio following complete resection of thymoma. J Cardiothorac Surg 2018; 13(1):1-9. [ Google Scholar]
- Mizunuma M, Yokoyama Y, Futagami M, Aoki M, Takai Y, Mizunuma H. The pretreatment neutrophil-to-lymphocyte ratio predicts therapeutic response to radiation therapy and concurrent chemoradiation therapy in uterine cervical cancer. Int J Clin Oncol 2015; 20(5):989-96. [ Google Scholar]
- Chun S, Shin K, Kim KH, Kim HY, Eo W, Lee JY, Namkung J, Kwon SH, Koh SB, Kim HB. The neutrophil-Lymphocyte ratio predicts recurrence of cervical intraepithelial neoplasia. J Cancer 2017; 8(12):2205. [ Google Scholar]
- Kolben TM, Etzel LT, Bergauer F, Hagemann I, Hillemanns P, Repper M. A randomized trial comparing limited-excision conisation to Large Loop Excision of the Transformation Zone (LLETZ) in cervical dysplasia patients. J Gynecol Oncol 2019; 30(3):e42. [ Google Scholar]