J Res Health Sci. 22(2):e00550.
doi: 10.34172/jrhs.2022.85
Original Article
Risk Assessment of Silicosis and Lung Cancer Mortality associated with Occupational Exposure to Crystalline Silica in Iran
Nafiseh Nasirzadeh 1, Zahra Soltanpour 2, Yousef Mohammadian 2, *, Farough Mohammadian 3
Author information:
1Department of Occupational Health Engineering, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
2Department of Occupational Health Engineering, Faculty of Health, Tabriz University of Medical Science, Tabriz, Iran
3Department of Occupational Health Engineering, Environmental Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran
Abstract
Background: Exposure to crystalline silica has long been identified to be associated with lung diseases. Therefore, the present study aimed to assess the risk of silicosis and lung cancer associated with occupational exposure to crystalline silica in Iran.
Study Design: It is a systematic review study.
Methods: Different databases were searched, and the Cochrane method was used for the systematic review. Thereafter, cumulative exposure to crystalline silica (mg/m3 -y) was calculated in every industry. The relative risk of death from silicosis was performed using Mannetje’s method. Based on the geometric mean of exposure, the lung cancer risk of exposure to crystalline silica was also calculated.
Results: As evidenced by the results, worker’s exposure to silica ranged from a geometric mean of 0.0212- 0.2689 mg/m3 (Recommended standard by the American Conference of Governmental Industrial Hygienists (ACGIH) was 0.025 mg/m3 ), which is generally higher than the occupational exposure limit recommended by National Institute for Occupational Safety and Health (NIOSH), ACGIH, and occupational exposure limits. The relative risk of silicosis was in the range of 1 to 14 per 1000 people, and the risk of lung cancer in workers ranged from 13-137 per 1000 people.
Conclusion: Since workers are at considerable risk of cancer due to exposure to silica in Iran, exposure control programs need to be implemented in workplaces to decrease the concentration of silica.
Keywords: Crystalline silica, Exposure, Lung cancer risk Systematic review
Copyright and License Information
© 2022 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Nasirzadeh N, Soltanpour Z, Mohammadian Y, Mohammadian F. Risk assessment of silicosis and lung cancer mortality associated with occupational exposure to crystalline silica in iran. J Res Health Sci. 2022; 22(2):e00550. doi:10.34172/jrhs.2022.85
Background
Crystalline silica is the second most common mineral, existing in more than 90% of the earth’s crust1; therefore, sand, rock, and soil have the most abundant crystalline silica.2 Workers are exposed to crystalline silica in mining, smelting, sandblasting, building, and glass industries.3 Previously published studies demonstrated that masons, plasters, and miners had the highest exposure to crystalline silica.4,5 The respiratory system is known as the primary pathway of exposure to crystalline silica dust.6 Exposure to crystalline silica has long been identified to be associated with lung diseases,7 such as silicosis which is a well-known lung disease.8
Exposure to higher concentrations of crystalline silica can cause “acute silicosis” which has a high mortality.9 “Chronic silicosis” is the most common form of pulmonary fibrosis among crystalline silica-exposed workers.2 The studies have suggested that pulmonary fibrosis can elevate the risk of lung cancer.10 International Agency for Research on Cancer (IARC) has introduced crystalline silica in the form of quartz or cristobalite as a human carcinogen.11 Workers are exposed to a low concentration of crystalline silica in workplaces; nonetheless, they are faced with a significant risk of cancer.12
There are an estimated 23 million crystalline silica-exposed workers in China13; moreover, over three million in India14 and over two million employees in the United States15 are exposed to crystalline silica. Annually, almost 800 workers die from lung cancer as a result of inhaling crystalline silica in Britain.16 The published studies have reported that workers in developing countries are exposed to crystalline silica in workplaces.17
Recently, risk assessment has become one of the most important aspects in the management of occupational diseases.18 There is a dearth of research on the assessment of the risk of lung cancer due to exposure to crystalline silica.18-21 Some studies have collected quantitative exposure data for the estimation of risk, for instance, Mannetje et al in IARC used a quantitative method for estimating the rate of silicosis mortality in six cohort studies and reported that the rate of silicosis mortality was above the risk of 1 per 1000 typically deemed acceptable by the Occupational Safety and Health Administration (OSHA).22 In the other study, Steenland et al examined lung cancer in 10 silica-exposed cohorts and indicated that the estimated excess lifetime risk of lung cancer for a worker exposed from age 20 to 65 at 0.1 mg/m3 crystalline silica (the permissible level in many countries) was 1.1%-1.7% (The background lifetime risk of death from lung cancer is 3%-6%.).23 In Iran, Azari et al assessed the relative risk of death from silicosis and lung cancer in traditional brick production and reported that this risk was in the range of 1-63.6 per 1000 people, and the risk of lung cancer was 124.08 per 1000 people.24
There is not any organized and comprehensive study on the status of exposure to crystalline silica and its health risk in Iranian workplaces. Therefore, the present study aimed to provide a systematic review of exposure to crystalline silica in all silica-related industries, as well as the estimation of the risk of silicosis and lung cancer due to exposure to crystalline silica.
Methods
Search strategy
All of the available studies in the field of occupational exposure to crystalline silica, including case-control and cohort studies, were provided.The literature search strategy was conducted using the following keywords: «Silica», “Crystalline silica», «Exposure”, «Occupational exposure», “Industrial», «Workplace», «Factory”, and “Iran”. All of the articles that reported the concentration of crystalline silica in air samples, as well as those published in English and Persian languages, were selected for the study. Due to the numerous applications of silica in recent decades, the query was carried out from 2000-2021. The Cochrane review method was used as a guideline for the systematic review.25,26 According to this method, PECO (Participants, Exposure, Comparators, and Outcomes) statement is as follows:
-
Participants: Humans, who had occupational exposure to crystalline silica
-
Exposure: Exposure to crystalline silica in silica-related industries
-
Comparators: People exposed to crystalline silica and other people
-
Outcomes: Increasing the concentration of crystalline silica in environmental or individual samples
Web of Science (WOS), Scopus, PubMed, Google Scholar, and SID (Scientific Information Database) were selected to implement the search strategy. In addition, the manual inspection of reference lists was used in order to gain access to more articles and reduce bias.
Screening of articles
The screening of articles was performed by title, abstract, and full text of the articles, separately. The inclusion criteria were all articles performed on occupational exposure to crystalline silica in Iran. On the other hand, the exclusion criterion entailed the articles on the biomonitoring of individuals. Moreover, abstracts (without their full-text available online), review and mini-review articles, conference papers, meta-analyses, modeling studies, books, and unpublished studies were excluded.
We used EndNote X9® (Thomson Reuters, Toronto, Canada) software27 to prepare the list of the articles and finally downloaded the full text of the screened articles. In order to reduce the error, search strategies were used by two researchers in this study separately. When there were disagreements, a third researcher was involved.
Data extraction
As illustrated in Table 1, data extraction was performed based on year, monitoring station number, mean and standard deviation concentration of crystalline silica, method of detection, city, occupation, and industrial activity.
Table 1.
Basic characteristics of the included studies
|
Year
|
Monitoring
station number
|
Mean±SD
|
Method of detection
|
City
|
Occupation
|
Industrial activity
|
Ref
|
| 2000 |
- |
2.62 ± 0.00 |
XRD |
Semnan |
Ferrosilicon |
Furnace |
28
|
| 2003 |
- |
0.49 ± 0.105 |
NIOSH7500 |
Arak |
Lead metal mining |
The mines |
29
|
| 2004 |
22 |
0.057 ± 0.016 |
NIOSH7500 |
Kashmar |
Mining |
The mines |
30
|
| 2007 |
40 |
0.86 ± 1.04 |
NIOSH7500 |
Hamadan |
Crushing |
Stone deformation operations |
31
|
| 2007 |
75 |
0.008 ± 0.004 |
Spectrophotometry |
Golestan |
Wheat flour producing |
Food industry |
32
|
| 2008 |
24 |
0.01 ± 0.005 |
NIOSH7500 |
Khaf |
Iron stone- Hammering |
Stone deformation operations |
33
|
| 2008 |
24 |
1.48 ± 0.39 |
NIOSH7500 |
Khaf |
Iron stone- Excavation |
Mines |
33
|
| 2009 |
10 |
0.275 ± NM |
NIOSH7602 |
East-Tehran |
Stone cutting and milling |
Stone deformation operations |
3
|
| 2009 |
10 |
0.343 ± NM |
NIOSH7602 |
East-Tehran |
Foundry work |
Foundry |
3
|
| 2009 |
10 |
0.132 ± NM |
NIOSH7602 |
East-Tehran |
Glass manufacturing |
Glass manufacturing |
3
|
| 2009 |
10 |
0.267 ± NM |
NIOSH7602 |
East-Tehran |
Asphalting |
Asphalt manufacturing |
3
|
| 2009 |
10 |
0.193 ± NM |
NIOSH7602 |
East-Tehran |
Construction |
Construction |
3
|
| 2009 |
10 |
0.261 ± NM |
NIOSH7602 |
East-Tehran |
Sand and gravel mining |
Sand and gravel production |
3
|
| 2009 |
10 |
0.272 ± NM |
NIOSH7602 |
East-Tehran |
Sandblasting |
Sandblast |
3
|
| 2009 |
10 |
0.328 ± NM |
NIOSH7602 |
East-Tehran |
Ceramic manufacturing |
Tile and ceramic industry |
3
|
| 2009 |
10 |
0.160 ± NM |
NIOSH7602 |
East-Tehran |
Bricks manufacturing |
Bricks manufacturing |
3
|
| 2009 |
10 |
0.220 ± NM |
NIOSH7602 |
East-Tehran |
Cement manufacturing |
Cement manufacturing |
3
|
| 2011 |
50 |
0.29 ± 0.039 |
NIOSH 7601 |
Tehran |
Metro excavating |
Excavations |
34
|
| 2011 |
25 |
0.164 ± 0.112 |
NIOSH7601 |
- |
Glass sandblasting |
Sandblast |
35
|
| 2011 |
5 |
15.5 ± 0.00 |
NIOSH7501 |
Mashhad |
Iron stone |
Mines |
36
|
| 2012 |
48 |
0.34 ± 0.11 |
NIOSH7602 |
Mazandaran |
Foundry |
Foundry |
37
|
| 2012 |
48 |
0.19 ± 0.13 |
NIOSH7602 |
Mazandaran |
Brick industry |
Brick industry |
37
|
| 2012 |
48 |
0.28 ± 0.10 |
NIOSH7602 |
Mazandaran |
Sand and gravel production |
Sand and gravel production |
37
|
| 2012 |
48 |
0.24 ± 0.17 |
NIOSH7602 |
Mazandaran |
Asphalting |
Asphalt industry |
37
|
| 2013 |
4 |
0.04 ± 0.02 |
NIOSH7601 |
Pakdasht |
Foundry |
Foundry |
38
|
| 2014 |
8 |
0.21 ± 0.19 |
NIOSH7500 |
- |
Tile industry |
Tile and ceramic industry |
39
|
| 2014 |
60 |
0.19 ± 0.138 |
NIOSH7601 |
Tehran |
Demolition of buildings |
Construction |
40
|
| 2015 |
22 |
0.088 ± 0.055 |
NIOSH7601 |
Pakdasht |
Foundry |
Foundry |
41
|
| 2015 |
12 |
0.589 ± 3.04 |
NIOSH7500 |
Khuzestan |
Cement Company |
Cement production |
42
|
| 2016 |
55 |
0.246 ± 0.047 |
NIOSH7602 |
- |
Mining |
Mines |
43
|
| 2016 |
60 |
0.25 ± 0.13 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
20
|
| 2016 |
5 |
0.13 ± 0.019 |
NIOSH7602 |
- |
Construction |
Construction |
44
|
| 2016 |
44 |
0.17 ± 0.79 |
NIOSH7602 |
Dorud |
Sand washing |
Sand and gravel production |
45
|
| 2016 |
96 |
0.313 ± 0.180 |
NIOSH7602 |
Mazandaran |
Sandblasting |
Sandblasting |
21
|
| 2016 |
96 |
0.169 ± 0.065 |
NIOSH7602 |
Mazandaran |
Ceramic manufacturing |
Tile and ceramic industry |
21
|
| 2016 |
96 |
0.282 ± 0.095 |
NIOSH7602 |
Mazandaran |
Sanding and graveling |
Sand and gravel production |
21
|
| 2016 |
96 |
0.194 ± 0.130 |
NIOSH7602 |
Mazandaran |
Brick producing |
Brick production |
21
|
| 2016 |
96 |
0.239 ± 0.171 |
NIOSH7602 |
Mazandaran |
Asphalt manufacturing |
Asphalt manufacturing |
21
|
| 2016 |
96 |
0.338 ± 0.110 |
NIOSH7602 |
Mazandaran |
Foundry |
Foundry |
21
|
| 2016 |
96 |
0.125 ± 0.093 |
NIOSH7602 |
Mazandaran |
Glass manufacturing |
Glass manufacturing |
21
|
| 2016 |
96 |
0.318 ± 0.120 |
NIOSH7602 |
Mazandaran |
Stone cutting & milling |
Stone deformation operations |
21
|
| 2016 |
55 |
0.27 ± 0.11 |
NIOSH7601 |
- |
Insulator manufacturing |
Insulator industry |
46
|
| 2016 |
114 |
1.02 ± 0.17 |
NIOSH7601 |
East-Iran |
Mines |
Mines |
47
|
| 2017 |
40 |
0.297 ± 272 |
NIOSH7602 |
Tehran |
Machine brick producing |
Bricks manufacturing |
24
|
| 2017 |
5 |
0.045 ± 0.03 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
20
|
| 2017 |
11 |
0.052 ± 0.025 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
20
|
| 2017 |
14 |
0.041 ± 0.014 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
20
|
| 2017 |
7 |
0.024 ± 0.008 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
20
|
| 2017 |
12 |
0.039 ± 0.02 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
20
|
| 2017 |
127 |
0.507 ± 0.23 |
NIOSH7601 |
Save |
Insulator |
Insulator industry |
48
|
| 2017 |
30 |
0.507 ± 0.23 |
NIOSH7601 |
- |
Insulator |
Insulator industry |
48
|
| 2017 |
55 |
0.25 ± 0.05 |
NIOSH7602 |
- |
Foundry |
Foundry |
49
|
| 2017 |
6 |
0.17 ± 0.02 |
NIOSH7602 |
- |
Automobile manufacturing |
Machine production |
19
|
| 2018 |
36 |
0.12 ± 0.3 |
NIOSH7500 |
Khorasan |
Cement manufacturing |
Cement industry |
50
|
| 2018 |
55 |
0.27 ± 0.05 |
NIOSH7601 |
- |
Insulator |
Insulator factories |
51
|
| 2018 |
5 |
0.223 ± 0.051 |
NIOSH7601 |
- |
Furnaces |
Furnace |
52
|
| 2018 |
5 |
0.218 ± 0.00 |
NIOSH7601 |
- |
Furnace |
Furnace |
52
|
| 2019 |
40 |
0.034 ± 0.037 |
NIOSH7601 |
Kermanshah |
Cement manufacturing |
Cement industry |
53
|
| 2020 |
72 |
0.027 ± 0.008 |
NIOSH7602 |
Nishabur |
Concreting |
Concrete Workers |
54
|
| 2020 |
30 |
0.651 ± 0.69 |
NIOSH7602 |
Tehran |
Traditional brick producing |
Bricks manufacturing |
24
|
Risk assessment
Prior to conducting risk assessment, we investigated the homogeneity of data; moreover, in order to detect and remove outliers, we used the box plot at a 95% confidence level. Mean and geometric standard deviation were calculated for every industrial activity. Thereafter, cumulative exposure to crystalline silica (mg/m3-y) (Mean of concentration × Years of exposure) was calculated for risk assessment. The relative risk of death from silicosis was determined using Mannetje’s method.23 In this method, the exposure history and crystalline silica concentration are two main factors. In addition, the exposures of all industrial workers in different studies were classified according to the Mannetje category for cumulative exposure.23Table 2 displays the exposure-related mortality rates and mortality rate ratios from silicosis in Mannetje’s method.
Table 2.
Relative risk of silicosis- related mortality in exposed workers according to their cumulative exposure (mg/m3-year) to crystalline silica in Mannetje’s method
|
Cumulative exposure to crystalline silica (mg/m
3
-y)
|
Relative risk (95% CI)
|
| 0-0.99 |
1.00 |
| 0.99- 1.97 |
3.39 (1.42, 8.08) |
| 1.97- 2.87 |
6.22 (2.56, 15.12) |
| 2.87- 4.33 |
9.40 (3.71, 23.80) |
| 4.33-7.12 |
13.69 (5.04, 37.18) |
| 7.12- 9.58 |
22.64 (7.88, 65.10) |
| 9.58- 13.21 |
23.97 (8.05, 71.32) |
| 13.21- 15.89 |
40.25 (13.25, 122.3) |
| 15.89-28.10 |
25.11 (8.09, 77.91) |
| > 28.10 |
63.63 (19.87, 203.8) |
The lung cancer risk of crystalline silica was calculated according to the model of Rice et al12 using formula 1. This model is based on the geometric mean of exposure to crystalline silica and 45 years of exposure. In this formula, (A) is the risk of death from lung cancer in workers, and (GM) denotes the geometric mean of exposure to crystalline silica.
A = 0.77 + 373.69 × GM (1)
Results
Based on the research reports of the databases, a total of 72 articles were published from September 2000 to September 2020 [PubMed (n = 28), Scopus (n = 8), WOS (n = 5), SID (n = 24), and other databases (n = 7)]. Due to duplication, 15 articles were ruled out. Finally, 36 papers were selected for the study and analyzed by the Preferred Reporting Items for Overviews of Reviews (PRIOR) method (Figure 1). A total of 24 articles were published in Persian. A number of 1, 421 measuring stations in various industries were investigated in 36 studies conducted in the field of worker exposure in Iran. As presented in Table 1, the studies were conducted in eight provinces, including Markazi, Razavi Khorasan, Hamadan, Golestan, Tehran, Mazandaran, Khuzestan, and Lorestan, as well as 13 cities, namely Arak, Save, Kashmar, Khaf, Nishabur, Hamadan, a city in Golestan, Tehran, Pakdasht, a city in Mazandaran, a city in Khorasan, Khuzestan, Dorud. The majority of studies were managed in Razavi Khorasan province (n = 4).
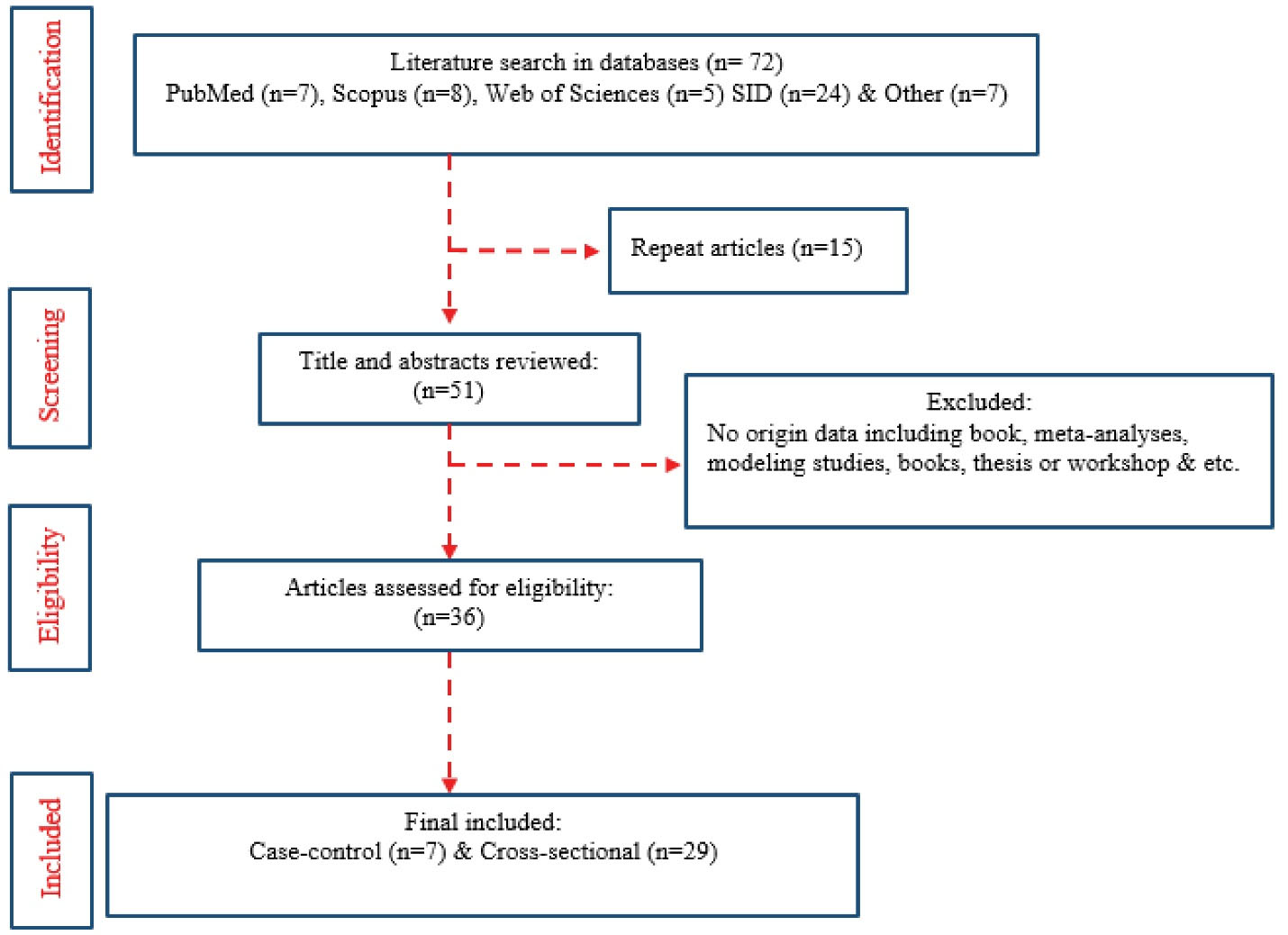
Figure 1.
Preferred Reporting Items for Overviews of Reviews displaying selected literature reviews.
.
Preferred Reporting Items for Overviews of Reviews displaying selected literature reviews.
The studies were performed in 17 industrial activities, such as cement manufacturing, mining, construction, foundry, furnace, stone deformation, glass manufacturing, asphalt manufacturing, sand and gravel production, sandblast, tile, and ceramic industry, brick production, insulator industry, excavation, concrete, food industry, and machine industry. Most studies were performed in mines and foundries (n = 6). One study was carried out in the food industry and another in machine industry. The box plot demonstrated that four studies encompassed outliers. As depicted in Table 1, these data were highlighted by Italic font.28,33,36,47 Outliers were deleted and not used in risk assessment; therefore, 2, 036 measuring stations in various industries were selected from 32 studies for risk assessment. In most studies, laborers worked six days a week and their working hours were more than 8 hours.
The geometric mean concentration for workers’ exposure to crystalline silica ranged from 0.0212-0.2689 mg/m3 (Table 3). In addition, the mean concentration of crystalline silica was obtained at 0.1476 ± 0.1628 in Iranian industries, which is higher than recommended exposure standard limit by the American Conference of Governmental Industrial Hygienists (ACGIH), Iran’s national occupational exposure limits (0.025 mg/m3),55 NIOSH (0.05 mg/m3),56 as well as OSHA (0.01 mg/m3).57
Table 3.
Mean concentrations of exposure to crystalline silica in various industrial activities in Iran
|
Industrial activity
|
Number of samples
|
Mean and arithmetic
standard deviation
|
Mean and geometric
standard deviation
|
| Cement manufacturing |
98 |
0.2408 ± 0.2443 |
0.1516 ± 0.2116 |
| The mines |
(77 + NM)a |
0.2643 ± 0.2171 |
0.1901 ± 0.1772 |
| Construction |
75 |
0.1710 ± 0.0356 |
0.1683 ± 0.0290 |
| Foundry |
235 |
0.2332 ± 0.1365 |
0.1806 ± 0.1246 |
| Furnace |
10 |
0.2205 ± 0.0035 |
0.2205 ± 0.0025 |
| Stone deformation operations |
170 |
0.3658 ± 0.3565 |
0.1656 ± 0.3087 |
| Glass manufacturing |
106 |
0.1285 ± 0.0049 |
0.1285 ± 0.0035 |
| Asphalt manufacturing |
154 |
0.2487 ± 0.0159 |
0.2483 ± 0.0129 |
| Sand and gravel production |
198 |
0.2483 ± 0.0530 |
0.2433 ± 0.0459 |
| Sandblast |
131 |
0.2496 ± 0.0769 |
0.2408 ± 0.0628 |
| Tile and ceramic industry |
114 |
0.2266 ± 0.0674 |
0.2357 ± 0.0825 |
| Bricks production |
189 |
0.2512 ± 0.2159 |
0.1605 ± 0.1970 |
| Insulator industry |
276 |
0.2005 ± 0.1912 |
0.1155 ± 0.1814 |
| Excavations |
50 |
0.2948 ± 0.1169 |
0.2689 ± 0.1046 |
| Concrete Workers |
72 |
0.0335 ± 0.0311 |
0.0212 ± 0.0291 |
| Others |
81 |
0.0890 ± 0.1146 |
0.0368 ± 0.0810 |
| Total |
1421 |
|
0.1476 ± 0.1628 |
aThe number of measuring stations was not mentioned in one of the studies that measured the concentration of silica in the mines.
As presented in Tables 1 and 2, workers in various industries were exposed to different grades of crystalline silica. In this study, we observed that iron-stone miners were exposed to the highest amount of crystalline silica (Table 1)33; nonetheless, to maintain homogeneity, the data related to the study by Naghizadeh et al on iron-stone miners were removed from the risk assessment process. It seems that health risk for iron-stone miners can be at the highest level; therefore, this issue needs more assiduous attention in the future. Furthermore, according to Table 3, workers in excavations are exposed to the highest concentration of crystalline silica (0.2689 ± 0.1046 mg/m3). The geometric mean concentration of crystalline silica was the lowest in the food industry (0.008 ± 0.004 mg/m3).
Discussion
Scarselli et al studied some workers potentially at risk of silica exposure selected from the Italian database of workplaces. They reported that the most involved sectors at high risk of silica exposure were construction, mining and quarrying, metalworking, and manufacturing of non-metallic products. In addition, they reported that workers in the manufacturing and construction industries were exposed to the highest level of crystalline silica.58 On the contrary, among the 16 industrial activities classified in this study, the manufacturing and construction industries were the eighth industries.
In 2015, according to OSHA compliance data from 1979 to 2015, Doney et al reported that workers in the poured concrete foundation had the highest exposure to crystalline silica. Moreover, out of 100 000 workers, 99.7% of cases were potentially exposed to crystalline silica at higher than the occupational exposure limit recommended by NIOSH in 2014.59 Concrete workers in Iran had the lowest mean airborne silica exposure levels (0.0212 ± 0.0291), which is lower than the occupational exposure limit recommended by NIOSH, ACGIH, and occupational exposure limits.
The relative risk of silicosis-related mortality based on Mannetje’s method and cumulative exposure categories was estimated to be in the range of 1-24 per 1000 people, ranging in the cumulative exposure categories of 0-0.99 to 9.58-13.21 in Mannetje’s method. In general, the mean rate of silicosis mortality in Iranian industries was 14 per 1000 people. These rates are above the risk of 1 per 1000 usually deemed acceptable by the US OSHA.3
According to Table 4, the risk of lung cancer due to exposure to crystalline silica based on the Rice model was in the range of 13-137 per 1000 people. In a 44-year cohort study on 34 018 workers, Liu et al reported the risk of lung cancer mortality as 128 per 1000 when the mean cumulative concentration (using a 25-year lag) was 0.01 to 1.12 mg/m3-y.60 In present study, most investigations were exposed-nonexposed studies. Since risk assessment is calculated by considering the history of exposure to silica, retrospective cohort studies may demonstrate more accurate estimations than other studies. The results of present study demonstrated that the risk of lung cancer was at the highest level among the stone deformation operations (1-137 per 1000). Inconsistent with this finding, Poinen-Rughooputh et al reported that miners were exposed to the highest risk of lung cancer mortality (in the range of 1-104 per 1000).61 Moreover, in present study, the lowest risk of lung cancer mortality was estimated in concrete workers in the range of 1-13 per 1000 people.
Table 4.
Risk of lung cancer mortality in exposed workers in different industries were calculated according to Rice et al. model
|
Industrial activity
|
Mean±(SD) (mg/m
3
)
|
Estimated excess lifetime risks of mortality from lung cancer
|
| Cement manufacturing |
0.2408 ± 0.2443 |
91 |
| The mines |
0.2643 ± 0.2171 |
100 |
| Construction |
0.171 ± 0.0356 |
65 |
| Foundry |
0.2332 ± 0.1365 |
88 |
| Furnace |
0.2205 ± 0.0035 |
83 |
| Stone deformation operations |
0.3658 ± 0.3565 |
137 |
| glass manufacturing |
0.1285 ± 0.0049 |
49 |
| Asphalt manufacturing |
0.2487 ± 0.0159 |
94 |
| sand and gravel production |
0.2483 ± 0.0530 |
94 |
| Sand blast |
0.2496 ± 0.0769 |
94 |
| Tile and ceramic industry |
0.2266 ± 0.0674 |
85 |
| Bricks production |
0.2512 ± 0.2159 |
94 |
| Insulator industry |
0.2005 ± 0.1912 |
76 |
| Excavations |
0.2948 ± 0.1169 |
111 |
| Concrete Workers |
0.0335 ± 0.0311 |
13 |
| Others |
0.0368 ± 0.081 |
15 |
In 2016, in a meta-analysis study, based on worldwide studies up to April 2016, the highest pooled concentration mortality ratio of exposure to crystalline silica was estimated at 6.03 (95% CI: 5.29-6.77) in mixed industries of Japan. Moreover, Italy had the highest number of observed lung cancer deaths (798 cases) before 2006.61 In their study, although the estimated health risk was high in Asian countries after Canada, the studies in Iran have been neglected. According to the results of the current research, the risk of both silicosis and lung cancer mortality is high in Iranian industries, and even numerous studies were conducted before 2016 in Iran.
Among the notable limitations of this study, we can refer to incomplete information on workers of all industries; therefore, we could not estimate the risk of mortality based on the percentage of exposed workers in industries. The expression of mortality based on the percentage of exposed cases can provide a better understanding of the hazard. Due to the high risk of silicosis and lung cancer mortality, it seems that the prevalent occupational health engineering strategies are not sufficient to protect workers; therefore, workers’ exposure to crystalline silica dust should be controlled in Iranian workplaces.
Conclusion
The authors provided a lung cancer risk assessment of occupational exposure to crystalline silica in Iranian industrials based on the collected quantitative exposure data. As evidenced by the obtained results, occupational exposure to crystalline silica was higher than occupational exposure limits. Furthermore, the relative risk of death from silicosis was in the range of 1-24 per 1000 people, and the risk of lung cancer ranged from 13-137 per 1000 people. It seems that the prevalent occupational health engineering strategies are not sufficient to protect workers; therefore, workers’ exposure to crystalline silica dust should be controlled in Iranian workplaces.
Highlights
-
The present study estimated silicosis and lung cancer caused by crystalline silica.
-
Workers’ exposure to crystalline silica ranged from 0.0212-0.2689 mg/m3.
-
This range was higher than the recommended standard limit by ACGIH (0.025 mg/m3).
-
The relative risk of silicosis mortality was in the range of 1-14 per 1000.
Acknowledgments
We would like to express our special appreciation for Dr. Mohammad Asghari Jafarabadi, Professor of Biostatistics, Tabriz University of Medical Sciences, Iran, who helped to analyze data in this study. Their willingness to give their time so kindly is very much appreciated.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
The study was based on the literature search and was not an experimental study; therefore, there was no need for ethics committee approval.
Funding
No funding was received.
References
- Yaroshevsky AA. Abundances of chemical elements in the Earth’s crust. Geochem Int 2006; 44(1):48-55. doi: 10.1134/s001670290601006x [Crossref] [ Google Scholar]
- Möhner M, Pohrt A, Gellissen J. Occupational exposure to respirable crystalline silica and chronic non-malignant renal disease: systematic review and meta-analysis. Int Arch Occup Environ Health 2017; 90(7):555-74. doi: 10.1007/s00420-017-1219-x [Crossref] [ Google Scholar]
- Rezazadeh Azari M, Rokni M, Salehpour S, Mehrabi Y, Jafari MJ, Naser Moaddeli A. Risk assessment of workers exposed to crystalline silica aerosols in the east zone of Tehran. Tanaffos 2009; 8(3):43-50. [ Google Scholar]
- Sanjel S, Khanal SN, Thygerson SM, Carter W, Johnston JD, Joshi SK. Exposure to respirable silica among clay brick workers in Kathmandu valley, Nepal. Arch Environ Occup Health 2018; 73(6):347-50. doi: 10.1080/19338244.2017.1420031 [Crossref] [ Google Scholar]
- Hoy RF, Chambers DC. Silica-related diseases in the modern world. Allergy 2020; 75(11):2805-17. doi: 10.1111/all.14202 [Crossref] [ Google Scholar]
- Liu Y, Wei H, Tang J, Yuan J, Wu M, Yao C. Dysfunction of pulmonary epithelial tight junction induced by silicon dioxide nanoparticles via the ROS/ERK pathway and protein degradation. Chemosphere 2020; 255:126954. doi: 10.1016/j.chemosphere.2020.126954 [Crossref] [ Google Scholar]
- Barnes H, Goh NSL, Leong TL, Hoy R. Silica-associated lung disease: an old-world exposure in modern industries. Respirology 2019; 24(12):1165-75. doi: 10.1111/resp.13695 [Crossref] [ Google Scholar]
- Leso V, Fontana L, Romano R, Gervetti P, Iavicoli I. Artificial stone associated silicosis: a systematic review. Int J Environ Res Public Health 2019; 16(4):568. doi: 10.3390/ijerph16040568 [Crossref] [ Google Scholar]
- t Mannetje A, Steenland K, Checkoway H, Koskela RS, Koponen M, Attfield M, Chen J, Hnizdo E, DeKlerk N, Dosemeci M. Development of quantitative exposure data for a pooled exposure-response analysis of 10 silica cohorts. Am J Ind Med 2002; 42(2):73-86. doi: 10.1002/ajim.10097 [Crossref] [ Google Scholar]
- Lacasse Y, Martin S, Gagné D, Lakhal L. Dose-response meta-analysis of silica and lung cancer. Cancer Causes Control 2009; 20(6):925-33. doi: 10.1007/s10552-009-9296-0 [Crossref] [ Google Scholar]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, International Agency for Research on Cancer, World Health Organization. Silica, Some Silicates, Coal Dust and Para-Aramid Fibrils. Geneva: WHO; 1997.
- Rice FL, Park R, Stayner L, Smith R, Gilbert S, Checkoway H. Crystalline silica exposure and lung cancer mortality in diatomaceous earth industry workers: a quantitative risk assessment. Occup Environ Med 2001; 58(1):38-45. doi: 10.1136/oem.58.1.38 [Crossref] [ Google Scholar]
- Chen W, Liu Y, Wang H, Hnizdo E, Sun Y, Su L. Long-term exposure to silica dust and risk of total and cause-specific mortality in Chinese workers: a cohort study. PLoS Med 2012; 9(4):e1001206. doi: 10.1371/journal.pmed.1001206 [Crossref] [ Google Scholar]
- Anlar HG, Bacanli M, İritaş S, Bal C, Kurt T, Tutkun E. Effects of occupational silica exposure on oxidative stress and immune system parameters in ceramic workers in Turkey. J Toxicol Environ Health A 2017; 80(13-15):688-96. doi: 10.1080/15287394.2017.1286923 [Crossref] [ Google Scholar]
- Bang KM, Mazurek JM, Wood JM, White GE, Hendricks SA, Weston A. Silicosis mortality trends and new exposures to respirable crystalline silica - United States, 2001-2010. MMWR Morb Mortal Wkly Rep 2015; 64(5):117-20. [ Google Scholar]
- Ahadzi DF, Afitiri AR, Ekumah B, Kanatey V, Afedzi A. Self-reported disease symptoms of stone quarry workers exposed to silica dust in Ghana. Health Sci Rep 2020; 3(4):e189. doi: 10.1002/hsr2.189 [Crossref] [ Google Scholar]
- Moyo D, Kgalamono S. Diagnostic challenges of silico-tuberculosis in a case with progressive massive fibrosis &#x 2013; a Zimbabwe case report. Occupational Health Southern Africa 2017; 23(1):11-3. doi: 10.10520/EJC-58434ef2c [Crossref] [ Google Scholar]
- Tanvi Newaz M, Ershadi M, Carothers L, Jefferies M, Davis P. A review and assessment of technologies for addressing the risk of falling from height on construction sites. Saf Sci 2022; 147:105618. doi: 10.1016/j.ssci.2021.105618 [Crossref] [ Google Scholar]
- Harati B, Shahtaheri SJ, Karimi A, Azam K, Ahmadi A, Afzali Rad M. Risk assessment of chemical pollutants in an automobile manufacturing. J Health Saf Work 2017; 7(2):121-30. [ Google Scholar]
- Mohammadi H, Golbabaei F, Farhang Dehghan, Normohammadi M. Occupational exposure assessment to crystalline silica in an insulator industry: Determination the risk of mortality from silicosis and lung cancer. J Health Saf Work 2017; 7(1):45-52. [ Google Scholar]
- Rokni M, Mohammadyan M, Hashemi ST, Asadi SM, Boogaard PJ, Heibati B. Risk assessment of workers exposed to crystalline silica aerosols. Hum Ecol Risk Assess 2016; 22(8):1678-86. doi: 10.1080/10807039.2016.1217391 [Crossref] [ Google Scholar]
- t Mannetje A, Steenland K, Attfield M, Boffetta P, Checkoway H, DeKlerk N. Exposure-response analysis and risk assessment for silica and silicosis mortality in a pooled analysis of six cohorts. Occup Environ Med 2002; 59(11):723-8. doi: 10.1136/oem.59.11.723 [Crossref] [ Google Scholar]
- Steenland K, Mannetje A, Boffetta P, Stayner L, Attfield M, Chen J. Pooled exposure-response analyses and risk assessment for lung cancer in 10 cohorts of silica-exposed workers: an IARC multicentre study. Cancer Causes Control 2001; 12(9):773-84. doi: 10.1023/a:1012214102061 [Crossref] [ Google Scholar]
- Rezazadeh Azari M, Sahatfardi F, Zarei F, Hariri AE, Salehpour S, Soori H. Risk assessment of mortality from silicosis and lung cancer in workers of machine factories and traditional brick production workshops with crystalline silica exposure. Occup Med 2020; 12:26-34. [ Google Scholar]
- Chandler J, Hopewell S. Cochrane methods - twenty years experience in developing systematic review methods. Syst Rev 2013; 2(1):76. doi: 10.1186/2046-4053-2-76 [Crossref] [ Google Scholar]
- Nasirzadeh N, Mohammadian Y, Fakhri Y. Concentration and cancer risk assessment of asbestos in Middle East countries: a systematic review-meta-analysis. Int J Environ Anal Chem 2020:1-15. doi: 10.1080/03067319.2020.1856375 [Crossref]
- Hupe M. EndNote X9. J Electron Resour Med Libr 2019; 16(3-4):117-9. doi: 10.1080/15424065.2019.1691963 [Crossref] [ Google Scholar]
- Dehdashti AR, Malek F. Silica dust exposure and respiratory effects in Semnan ferrosilicon workers. Koomesh 2000; 2(1):33-44. [ Google Scholar]
- Samadi S, Janid BS. Assessment of total dust and silica in lead metal mines. Feyz 2003; 28:84-9. [ Google Scholar]
- Golbabaei F, Barghi MA, Sakhaei M. Evaluation of workers’ exposure to total, respirable and silica dust and the related health symptoms in Senjedak stone quarry, Iran. Ind Health 2004; 42(1):29-33. doi: 10.2486/indhealth.42.29 [Crossref] [ Google Scholar]
- Aliabadi M, Bahrami B, Mahjub H, Ghorbani F, Barghi MA, Golbabaie F. Evaluation of free silica emission in ambient air of stone crushing in Azandarian area of Hamadan state by using of X-ray diffraction method. Avicenna J Clin Med 2007; 14(3):67-73. [ Google Scholar]
- Semnani S, Besharat S, Jabbari A, Keshtkar A, Abdollahi N. Determination of silica concentration in wheat flour produced in Golestan province. Gorgan Univ Med Sci 2007; 8:33-6. [ Google Scholar]
- Naghizadeh A, Mahvi A, Jabbari H, Dadpour A, Karimi M. Determination the level of dust ond free silica in air of Khaf iron stone quarries. Iran J Health Environ 2008; 1(1):37-44. [ Google Scholar]
- Kakoui H, Mousavi S, Panahi D, Rezazadeh Azari M, Hosseini M. Assessment of occupational exposure to total dust and crystalline silica in construction workers of metro, Tehran. J Health Saf Work 2012; 1(1):25-30. [ Google Scholar]
- Rezazadeh Azari M, Ramazani B, Mosavian MA, Movahedi M, Salehpour S. Serum malondialdehyde and urinary neopterin levels in glass sandblasters exposed to crystalline silica aerosols. Int J Occup Hyg 2011; 3(1):29-32. [ Google Scholar]
- Kakouei H, Sadegi N, Fani MJ, Rafieimanesh E, Golami A. Assessment of occupational exposure to crystalline silica dust in an iron-stone mine, and comparing the results with standards. International Journal of Basic Science in Medicine 2011; 3:45-54. [ Google Scholar]
- Mohammadyan M, Rokni M, Islami S, Fazeli A. Evaluation of workers’ exposure to crystaline silica particles in some factories of Mazandaran province. J Mazandran Univ Med Sci 2012; 22(88):17-24. [ Google Scholar]
- Kakui H, Ghasemkhani M, Omidiani Dost A, Rezazadeh Azari M, Rahimi A. Assessment of respirable dust exposure and free silica percent in small foundries (Less than 10 workers) in Pakdasht, 2011. Hakim Res J 2013; 16(3):211-9. [ Google Scholar]
- Askaripoor T, Kermani A, Pahlavan D, Jandaghi J, Kazemi E. Health risk assessment of occupational exposure to crystalline silica in a tile & ceramic Industry. Occup Med 2014; 6(2):44-53. [ Google Scholar]
- Kakoei H, Nourmohammadi M, Mohammadian Y, Zarei E, Zokaei M. Assessment of occupational exposure to crystalline silica during demolition of buildings in Tehran. Iran Occupational Health 2014; 11(2):63-9. [ Google Scholar]
- Omidianidost A, Ghasemkhani M, Azari MR, Golbabaei F. Assessment of occupational exposure to dust and crystalline silica in foundries. Tanaffos 2015; 14(3):208-12. [ Google Scholar]
- Sobhanardakani S, Saedi M. Assessment of particulate matter, free silica and toxic gases emissions from Khouzestan Cement Company. J Mazandaran Univ Med Sci 2015; 25(125):21-31. [ Google Scholar]
- Zarei F, Rezazadeh Azari M, Salehpour S, Khodakarim S, Kalantary S, Tavakol E. Exposure assessment of core making workers to respirable crystalline silica dust. J Health Saf Work 2017; 7(1):1-8. [ Google Scholar]
- Tavakol E, Rezazadeh Azari M, Salehpour S, Khodakarim S. Determination of construction workers’ exposure to respirable crystalline silica and respirable dust. J Saf Promot Inj Prev 2016; 3(4):263-70. [ Google Scholar]
- Parsaseresht GR, Rezazadeh Azari M, Zendehdel R, Hashemi Nazari S, Tavakol E. Evaluation of occupational exposure and biological monitoring of sand washing workers exposed to silica dusts. J Saf Promot Inj Prev 2016; 4(3):135-41. [ Google Scholar]
- Mohammadi H, Farhang Dehghan S, Golbabaei F, Ansari M, Yaseri M, Roshani S. Evaluation of serum and urinary neopterin levels as a biomarker for occupational exposure to crystalline silica. Ann Med Health Sci Res 2016; 6(5):274-9. doi: 10.4103/amhsr.amhsr_140_16 [Crossref] [ Google Scholar]
- Golbabaei F, Gholami A, Teimori-Boghsani G, Yaseri M, Kianmehr M. Evaluation of occupational exposure to silica dust in mining workers in eastern Iran. Open Environ Res J 2019; 12(1):1-6. doi: 10.2174/1874213001912010001 [Crossref] [ Google Scholar]
- Mohammadi H, Farhang Dehghan S, Golbabaei F, Roshani S, Pakzad R, Foroughi P. Pulmonary functions and health-related quality of life among silica-exposed workers. Tanaffos 2017; 16(1):60-7. [ Google Scholar]
- Zarei F, Rezazadeh Azari M, Salehpour S, Khodakarim S, Omidi L, Tavakol E. Respiratory effects of simultaneous exposure to respirable crystalline silica dust, formaldehyde, and triethylamine of a group of foundry workers. J Res Health Sci 2017; 17(1):e00371. [ Google Scholar]
- Mohammadyan M, Ahmadi Asour A, Pouransari M, Akrami R, Soroosh D, Razavi SM. Workers occupational exposure to free crystal silica of respirable particles in a cement factory in Khorasan Razavi province. J Sabzevar Univ Med Sci 2020; 27(1):65-72. [ Google Scholar]
- Mohammadi H, Farhang Dehghan S, Tahamtan A, Golbabaei F. Evaluation of potential biomarkers of exposure to crystalline silica: a case study in an insulator manufacturer. Toxicol Ind Health 2018; 34(7):491-8. doi: 10.1177/0748233718770073 [Crossref] [ Google Scholar]
- Shafiei-Alavijeh M, Rismanchian M. Evaluation of total and respirable dust and crystalline silica in the refractory process of metal melting furnaces. J Health Syst Res 2018; 14(2):189-94. doi: 10.22122/jhsr.v14i2.3142.[Persian] [Crossref] [ Google Scholar]
- Omidianidost A, Gharavandi S, Rezazadeh Azari M, Hashemian AH, Ghasemkhani M, Rajati F. Occupational exposure to respirable dust, crystalline silica and its pulmonary effects among workers of a cement factory in Kermanshah, Iran. Tanaffos 2019; 18(2):157-62. [ Google Scholar]
- Rahimi Moghadam S, Khanjani N, Mohamadyan M, Emkani M, Yari S, Layegh Tizabi MN. Changes in spirometry indices and lung cancer mortality risk estimation in concrete workers exposed io crystalline silica. Asian Pac J Cancer Prev 2020; 21(9):2811-7. doi: 10.31557/apjcp.2020.21.9.2811 [Crossref] [ Google Scholar]
- Dahlgren J, Wardenburg M, Peckham T. Goodpasture’s syndrome and silica: a case report and literature review. Case Rep Med 2010;2010. 10.1155/2010/426970
- NIOSH Hazard Review: Health Effects of Occupational Exposure to Respirable Crystalline Silica. Centers for Disease Control and Prevention; 2002.
- Occupational Safety and Health Administration (OSHA). Interim Enforcement Guidance for the Respirable Crystalline Silica in Construction Standard, 29 CFR 1926.1153. OSHA; 2019. Available from: https://www.osha.gov/laws-regs/standardinterpretations/2017-10-19. Updated October 19,2017. Accessed June 8, 2022.
- Scarselli A, Binazzi A, Marinaccio A. Occupational exposure to crystalline silica: estimating the number of workers potentially at high risk in Italy. Am J Ind Med 2008; 51(12):941-9. doi: 10.1002/ajim.20619 [Crossref] [ Google Scholar]
- Doney BC, Miller WE, Hale JM, Syamlal G. Estimation of the number of workers exposed to respirable crystalline silica by industry: analysis of OSHA compliance data (1979-2015). Am J Ind Med 2020; 63(6):465-77. doi: 10.1002/ajim.23109 [Crossref] [ Google Scholar]
- Liu Y, Steenland K, Rong Y, Hnizdo E, Huang X, Zhang H. Exposure-response analysis and risk assessment for lung cancer in relationship to silica exposure: a 44-year cohort study of 34,018 workers. Am J Epidemiol 2013; 178(9):1424-33. doi: 10.1093/aje/kwt139 [Crossref] [ Google Scholar]
- Poinen-Rughooputh S, Rughooputh MS, Guo Y, Rong Y, Chen W. Occupational exposure to silica dust and risk of lung cancer: an updated meta-analysis of epidemiological studies. BMC Public Health 2016; 16(1):1137. doi: 10.1186/s12889-016-3791-5 [Crossref] [ Google Scholar]