J Res Health Sci. 20(4):e00498.
doi: 10.34172/jrhs.2020.32
Original Article
Survival Percentile and Predictors of Difference in Survival among Hemodialysis Patients and Their Additive Interaction Using Laplace Regression
Salman Khazaei 1, 2, Mehdi Yaseri 2, Vida Sheikh 3, Maryam Nazemipour 4, Ebrahim Hazrati 5, Mohammad Ali Mansournia 2, *
Author information:
1Research Center for Health Sciences, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Epidemiology and Biostatistics, Tehran University of Medical Sciences, Tehran, Iran
3Clinical Research Development Unit of Shahid Beheshti Hospital, Hamadan University of Medical Sciences, Hamadan, Iran
4Psychosocial Health Research Institute, Iran University of Medical Sciences, Tehran, Iran
5Department of Anesthesiology, AJA University of Medical Sciences, Tehran, Iran
Abstract
Background: Identifying survival modifiable factors and additive interaction between them could help in prioritizing the clinical care of Hemodialysis (HD) patients. We aimed to examine the survival rate and its predictors in HD patients; and explore the additive interaction between survival modifiable factors.
Study design: A retrospective cohort study.
Methods: The present study was performed on 1142 HD patients in Hamadan Province, western Iran from 2007 to 2017. Data were collected through a researcher-made checklist on hospital records. Laplace regression was used to evaluate differences in 40th survival percentiles in different levels of predictors as well as exploring the pairwise additive interactions between variables.
Results: We observed significantly higher survival in nonsmoker patients (40th percentile difference = 5.34 months, 95% CI: 2.06, 8.61). Survival was shorter by more than 3 years in CRP positive patients (40th percentile difference=36.9 months, 95% CI: 32.37, 41.42). Patients with normal albumin (40th percentile difference =24.92, 95% CI: 18.04, 31.80) and hemoglobin (40th percentile difference = 18.65, 95% CI: 12.43, 24.86) had significantly higher survival (P<0.001). There was super-additive interaction between being CRP negative and nonsmoker (β3 = 9.42 months, 95% CI: 3.35, 15.49 (P=0.002)).
Conclusion: High CRP and low serum albumin and hemoglobin were associated with the increased risk of death in HD patients. The results of this study support the presence of super-additive interaction between CRP status with serum hemoglobin and also CRP status with smoking, resulting in excess survival in HD patients.
Keywords: Hemodialysis, Kidney failure, Survival, Laplace regression
Copyright and License Information
© 2020 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Citation: Khazaei S, Yaseri M, Sheikh V, Nazemipour M, Hazrati E, Mansournia MA. Survival Percentile and Predictors of Difference in Survival among Hemodialysis Patients and Their Additive Interaction Using Laplace Regression. J Res Health Sci. 2020; 20(4): e00498.
Introduction
Globally, chronic kidney disease (CKD) is a major health concern and an excessive cost of health care finances devoted to this problem
1
. The survival rate of these patients is lower than the general population, and it was not seen any improvement in their survival over recent years
2
.
Hemodialysis (HD) in Iran is generally used as the main choice for renal replacement therapy in end-stage renal disease (ESRD) patients and is provided free of charge in Iran
3
. Until now, limited studies have been performed in Iran regarding the survival of HD patients, indicating a low survival rate for these patients
4,5
.
According to litterateurs, age, ethnic background, level of serum albumin and hemoglobin, adequacy of dialysis, mean duration of dialysis per treatment session, renal replacement therapy method, body mass index (BMI), causes of kidney failure, and comorbidities with some diseases such as heart failure and cancer are considered as predictors of death in the HD patients
3,6-9
.
The interaction generally occurs as a result of the dependence of the influence of one risk factor to the presence of another risk factor. When there is additive interaction between the two risk factors that the patients with both risk factors simultaneously have higher risk of death than those expected based on summing the separate effects of the above-mentioned two risk factors
10
. Assessing interaction provides a better vision into the mechanisms for the occurrence of outcome and identify more beneficiary subgroups to be intervened when resources are limited. Therefore it is one of the stimulants for assessing additive interaction
10,11
. A strikingly increase showed in mortality risk among dialysis patients which was due to interaction between protein-energy wasting (PEW), cardiovascular diseases (CVD) and inflammation in patients
12
.
Identification of the additive interaction between survival modifiable factors could help in prioritizing the clinical care of HD patients. To our knowledge, there was no previous study done on the additive interaction between survival modifiable factors in hemodialysis patients, moreover, evidence about the survival of hemodialysis patients and its related factors in developing countries is limitedd.
Therefore, the purposes of the present study were (1) evaluating the survival rate and its predictors in HD patients in Hamadan province, and (2) investigating the additive interaction between the survival modifiable factors in HD patients.
Methods
Study Design
Retrospective cohort study
Settings and Participants
We examined data obtained from 1142 hemodialysis patients in Hamadan Province, western Iran in the period of 11 years from Mar 2007 to Mar 2017. Hamadan Province is located in the west of Iran and has an area of 19,493 square km in extent and 1,758,268 population according to the national census by the Statistical Center of Iran in 2011. Information was obtained from the eight hospitals of the province with dialysis centers including Alimoradian, Besat, Vali-asr, Ghaem, Imam Hossein, Valiasr, Shahid-Beheshti and Imam Reza in Nahavand, Hamadan, Tuyserkan, Asadabad, Malayer, Razan, Hamadan and Kabudarahang city, respectively.
Patients undergoing HD due to acute renal failure, patients undergoing peritoneal dialysis, patients on transient hemodialysis and patients who had incomplete medical records were not included in the study and were considered as exclusion criteria.
Clinical and Demographic Measures
Data were collected using a checklist on hospital records of all HD patients hospitalized in provincial hospitals. The checklist used in this study included characteristics related to demographic profiles (age, gender, marriage status, Body mass index (BMI), location, educational level, previous history of smoking or substance abuse), and patient biochemical and clinical information (Hemoglobin level, C-reactive protein (CRP) status (+/-), blood urea nitrogen (BUN), creatinine, urea reduction ratio (URR), sodium, phosphor, calcium, albumin and etiology of ESRD). Clinical and biochemical data at the time of diagnosis and before onset of the first dialysis were gathered for each patient as well and considered as baseline data. To minimize measurement variability, we averaged both baseline measures for each patient. These records were gathered by assessing patients’ medical records in the dialysis ward.
Outcomes
We considered death due to renal failure as the endpoint of the study. Patients with renal transplantation, withdrawal of dialysis, lost-to-follow-up, competing risks (patients who died due injury, accident, or other causes unrelated to renal failure) and those transferred to another dialysis facility out of province were treated as censored cases.
Analytical Methods
Laplace regression was used to evaluate differences in survival percentiles according to the levels of predictors and adjusting for potential confounders. Laplace regression as a flexible method can be used for computing the conditional percentiles of the time-to-event variables
13
. The time that the specific percentage of the investigated cases have experienced the outcome of interest can be considered as survival percentile for that time.
To avoid extrapolation, we examined the 40th percentile of survival time given that during the study period, death occurred for 43% of participants. Therefore, using Laplace regression, we estimated differences in the time duration by which the first 40% of the HD patients died according to the levels of predictors. We also assessed pairwise, additive interactions between predictors.
To assess the effect of the two binary predictors (e.g. G and E) and their additive interaction on the 40th survival percentile (p(40)), we fitted the following Laplace model:
"T(p(40)│G,E)=β_0 (p(40))+β_1 (p(40))G+β_2 (p(40))E+β_3 (p(40)).G.E"
According to the above equation the measure of additive interaction between two predictors is the parameter β3(p(40)). If β3(p(40)) >0, superadditive interaction between two predictors exists and If β3(p(40)) <0, interaction is subadditive
14
.
We analyzed the data using Stata software version 12 (Stata Corp LP, College Station, Texas) at less than 5% significant level.
Ethical approval
The Ethics Committee of Tehran University of Medical Sciences (TUMS.SPH.REC.1395.1300) approved our study. To keep confidentiality, all patients identifier were removed.
Results
The baseline characteristics of HD patients are shown in Table 1. Of the 1142 HD patients, 617 (54.03%) were male, 717 (62.78%) were urban resident and 928 (81.26%) of them were married. The mean age (SD) at diagnosis and the mean BMI (SD) of patients was 55.52 (14.65) year and 23.26 (3.54) kg/m2, respectively. Among all the subjects; 256 (22.42%) were smokers and 385 (34.65%) were CRP positive at diagnosis. Mean hemoglobin, sodium, phosphor, calcium and serum albumin of patients were 10.60 mg/dl, 138.76 mEq/L, 5.15 mg/dl, 8.75 mg/dl and 3.66 g/dl, respectively.
Survival time of patients
Laplace regression results showed that the 10, 20, 30 and 40 percent of the investigated HD patients died in the 5.63, 13.43, 22.27 and 33.13 months after the diagnosis, respectively. The effect of prognostic factors on patient’s survival has been demonstrated in Table 1. Based on multivariable Laplace regression, females had 3.3 months’ higher survival (40th percentile difference = 3.29 months, 95% CI: 0.69, 5.88). Urban residence patients had 2.65 months more survival compared with rural dwellers (40th percentile difference = 2.65 months, 95% CI: 0.50, 4.80). We observed a significantly higher survival in nonsmoker patients (40th percentile difference = 5.34 months, 95% CI: 2.06, 8.61). Survival was shortened by more than 3 years in CRP positive patients (40th percentile difference = 36.90 months, 95% CI: 32.37, 41.42). Patients with normal Albumin ≥3.5 g/dl) (40th percentile difference =24.92, 95% CI: 18.04, 31.80) and normal Hemoglobin ≥11 g/dl) (40th percentile difference = 18.65, 95% CI: 12.43, 24.86) had significantly higher survival (P<0.001).
Table 1.
40th Percentile in survival and its difference according to levels of predictors, in HD patients in Hamadan province, 2007-2017
|
Variables
|
No (%)
|
Time to death
(months)
|
Unadjusted Percentile
Difference (95% CI)
|
P
value
|
Adjusted
percentile
Difference (95% CI)
a
|
P
value
|
| Gender |
|
|
|
|
|
|
| Male |
617 (54.03) |
25.56 |
Ref. |
|
Ref. |
|
| Female |
525 (45.97) |
30.79 |
5.23 (-1.23,11.68) |
0.120 |
3.29 (0.69, 5.88) |
0.013 |
| Location |
|
|
|
|
|
|
| Urban |
717 (62.78) |
40.95 |
Ref. |
|
Ref. |
|
| Rural |
425 (37.22) |
35.3 |
5.65 (-0.52, 11.82) |
0.070 |
2.65 (0.50, 4.80) |
0.016 |
| Education (yr) |
|
|
|
|
|
|
| ≤9 |
939 (82.22) |
21.92 |
Ref. |
|
|
|
| >9 |
203 (17.78) |
31.89 |
9.97 (-0.06, 20.00) |
0.050 |
- |
- |
|
Body mass index (kg/m2)
|
|
|
|
|
|
|
| <25 |
820 (71.80) |
33.90 |
Ref. |
|
|
|
| ≥25 |
322 (28.20) |
36.07 |
2.17 (-5.10, 9.44) |
0.560 |
- |
- |
| Smoking |
|
|
|
|
|
|
| Yes |
256 (22.42) |
25.98 |
Ref. |
|
Ref. |
|
| No |
886 (77.58) |
34.97 |
8.99 (0.38, 17.61) |
0.040 |
5.34 (2.06, 8.61) |
0.001 |
| Albumin (g/dl) |
|
|
|
|
|
|
| <3.5 |
427 (39.28) |
10.57 |
Ref. |
|
Ref. |
|
| ≥3.5 |
660 (60.72) |
35.49 |
24.92 (18.04, 31.80) |
0.001 |
12.34 (9.02, 15.67) |
0.001 |
| Phosphor (mg/dl) |
|
|
|
|
|
|
| <3.5 |
114 (10.22) |
22.28 |
Ref. |
|
|
|
| ≥3.5 |
1002 (89.78) |
27.93 |
5.65 (-4.90, 16.19) |
0.290 |
- |
- |
| Calcium |
|
|
|
|
|
|
| <8.5 |
333 (29.73) |
29.94 |
Ref. |
|
|
|
| ≥8.5 |
787 (70.27) |
31.77 |
1.83 (-5.00, 8.68) |
0.600 |
- |
- |
|
Sodium
|
|
|
|
|
|
|
| <135 |
214 (19.18) |
34.12 |
Ref. |
|
|
|
| ≥135 |
902 (80.82) |
33.52 |
0.60 (-6.80, 800) |
0.880 |
- |
- |
| C-reactive protein |
|
|
|
|
|
|
| Positive |
385 (34.65) |
8.77 |
Ref. |
|
Ref. |
|
| Negative |
726 (65.35) |
45.67 |
36.90 (32.37, -41.42) |
0.001 |
16.46 (12.68, 20.23) |
0.001 |
| Dialysis weekly (hour) |
|
|
|
|
|
|
| <10 |
405 (35.46) |
23.40 |
Ref. |
|
|
|
| ≥10 |
737 (64.54) |
29.34 |
5.94 (-1.17, 31.00) |
0.110 |
- |
- |
| Hemoglobin (mg/dl) |
|
|
|
|
|
|
| <11 |
588 (53.60) |
16.63 |
Ref. |
|
Ref. |
|
| ≥11 |
509 (46.40) |
35.28 |
18.65 (12.43, 24.86) |
0.001 |
22.42 (18.10, 26.74) |
0.001 |
| Urea reduction ratio |
|
|
|
|
|
|
| <0.65 |
512 (49.04) |
24.22 |
Ref. |
|
|
|
| ≥0.65 |
532 (50.96) |
29.82 |
5.60 (-1.60, 12.76) |
0.130 |
- |
- |
a Adjusted for other variables in the model
The interaction between smoking and CRP status
The additive interaction between smoking (0 = smoker; 1 = never smoker) and CRP (0 = CRP positive; 1 = CRP negative) in predicting overall mortality were assessed. Predicted values of the 40th survival percentile for each of the four subgroups formed, calculated by combining the obtained coefficients estimates, have been shown in Table 2 and Figure 1a. The Laplace regression model indicated superadditive interaction in predicting the death between being nonsmoker and CRP negative: 9.42 months’ excess in 40th survival percentile for the effect of one predictor when the other predictor changes from 0 to 1. (β3 = 9.42 months, 95% CI: 3.35, 15.49 (P=0.002)).
The interaction between Hemoglobin level and CRP status
The interaction between Hemoglobin level (0 = Hb<11 mg/dl; 1 = Hb ≥11 mg/dl) and CRP status (0 = CRP positive; 1 = CRP negative) in predicting overall mortality in 40th survival percentile of HD patients has been shown in Table 3 and Figure 1b.
Table 2.
40th Survival percentiles (months), by levels of Smoking and CRP status
|
Variables
|
Smoker
|
Never smoker
|
Percentile
difference
|
| CRP Positive |
7.03 |
9.91 |
2.88 |
| CRP Negative |
37.15 |
49.45 |
12.30 |
| Percentile difference |
30.12 |
39.54 |
9.42 |
The estimate of the product term β3, suggested 5.26 additional months of 40th survival percentile for the effect of one variable when the level of the other one varies from 0 to 1 (β3 = 5.26 months, 95% CI: -3.31, 14.81 (P=0.21)). This excess in survival indicates the presence of superadditive interaction in predicting mortality between being normal hemoglobin level and CRP negative.
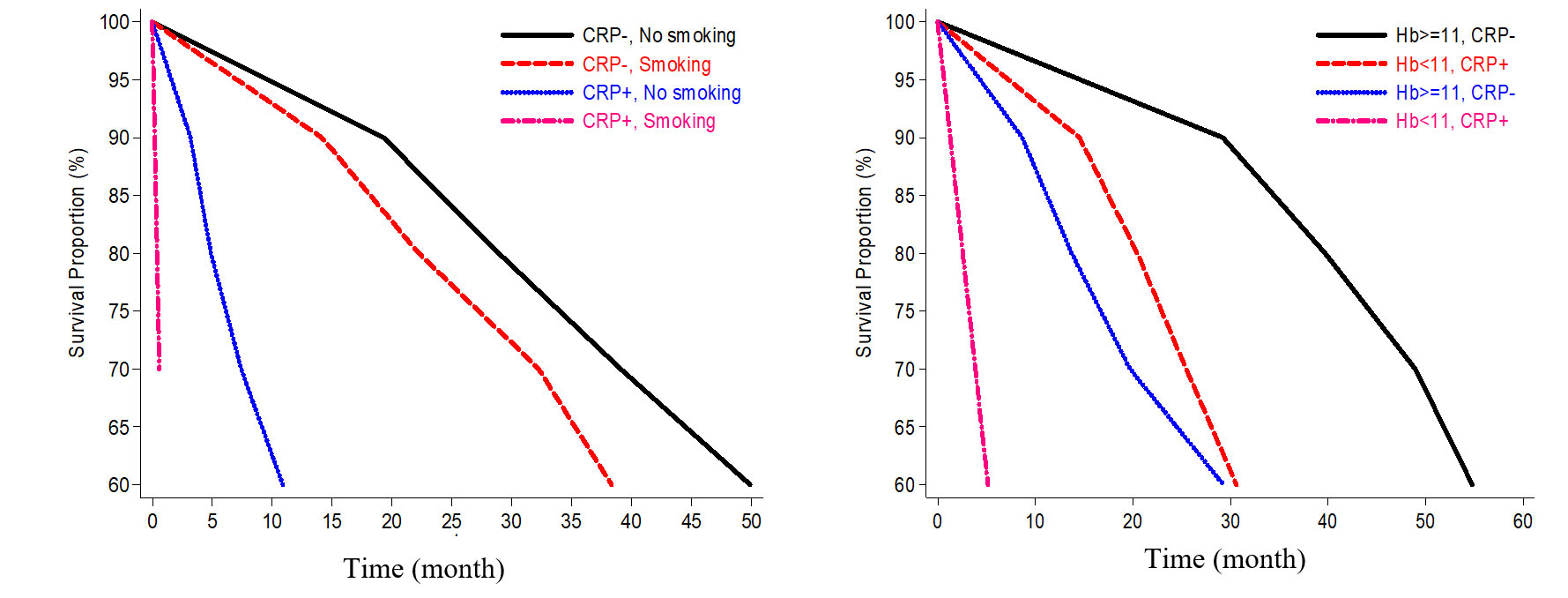
Figure 1.
Survival curves (according Laplace regression approach) by levels of a. smoking (smoker, never smoker) and CRP status (positive, negative); b. hemoglobin (<11 mg/dl, ≥11 mg/dl) and CRP status (positive, negative)
.
Survival curves (according Laplace regression approach) by levels of a. smoking (smoker, never smoker) and CRP status (positive, negative); b. hemoglobin (<11 mg/dl, ≥11 mg/dl) and CRP status (positive, negative)
Table 3.
40th Survival percentiles (months), by levels of Hemoglobin and CRP status
|
Variables
|
CRP Positive
|
CRP Negative
|
Percentile difference
|
| Hb<11 mg/dl |
7.40 |
29.80 |
22.40 |
| Hb ≥11 mg/dl |
26.40 |
54.07 |
27.67 |
| Percentile difference |
19.00 |
24.27 |
5.27 |
Discussion
Hemodialysis is a common treatment modality for ESRD patients in Iran. We investigated the predictors of survival in HD patients and explored the additive interaction between them in terms of survival. The findings of this study are useful as preliminary data for further studies in order to increase the quality care of HD patients. High CRP and low serum albumin and hemoglobin are independent predictors of mortality in HD patients. Being male, rural dweller and smoking were associated with a higher risk of mortality. There was an additive interaction between CRP and each of the variables serum hemoglobin and smoking on the (40th percentile of) survival.
In this regard, the low level of hemoglobin was associated with a higher risk of mortality in HD patients, which is consistent with our findings
15,16
. In a study, three-year survival rate of patients with Hb <9 g/dL was significantly lower than that for patients with Hb levels 10 to 11 g/dL (74.1% vs. 89.3%)
8
. The normal range of the hemoglobin level in HD patients is correlated with improving life quality
17
, cardiac and brain function
18,19
, decreasing hospitalization and treatment costs in these patients
20
.
In the present study, in agreement with several conducted observational studies, we found that low level of serum albumin was associated with poor survival
8,21,22
. Decreasing serum albumin levels with increasing time was associated with raising CVD related death
23
. In dialysis patients, hypoalbuminemia is applied as indicator of malnutrition and has a strong effect on mortality
24
.
Our findings revealed that the positive CRP was a strong predictor of death in HD patients. In consistence with our findings, several prospective studies have demonstrated CRP is an independent predictor for the future risk of death in these patients
25,26
. In general, inflammation is associated with wasting, oxidative stress, insulin resistance, endothelial dysfunction, and infections
17
. CRP can mediate processes involving in the development of atherosclerosis through plaque initiation, formation, and rupture, while it may not be merely a marker of inflammation
27
.
Our results showed a significant association between HD patients’ smoking and their survival rate, which was inconsistent with the findings of another study, which showed there was no significant relationship between smoking and survival rate
28
. A meta-analysis study reported a same results as our findings
29
.
Smoking as a modifiable risk factor for kidney failure through some mechanisms like excessive generation of free radicals, promoting atherosclerosis in renal arteries, and intra-renal hemodynamic changes
30,31
.
Additive interaction scale as a more relevant public health measure helps detect subgroups with the highest benefits from treatment
10
. The findings of this study support the presence of the super additive interaction between CRP status and serum Hemoglobin also CRP status and smoking. This finding is important because HD patients with a high mortality risk can be identified through regular screening. More studies are required to determine that multiple pathophysiological pathways may underlie these interaction effects.
Our study has suffered from some key limitations which had been inherited from existing data. Firstly, the absence of a Kt/V as an accurate reference method to estimate dialysis adequacy of patients. Second, due to its retrospective design, it was not possible to control data quality. Third, the addiction and smoking status of patients was based on their self-report and were prone to measurement bias. Fourth, the retrospective and observational nature of our analyses allowed the detection of associations, not causation. However, moderately large sample size, comprehensive clinical and laboratory evaluations and examining the additive interaction between the predictors of HD patient’s survival, can be considered as the strengths of our study.
Conclusion
High CRP and low serum albumin and hemoglobin are associated with the increased risk of death in HD patients, and male gender, rural dweller and smoking were significantly associated with a higher risk of mortality. The presence of super-additive interaction between CRP status and serum hemoglobin also CRP status and smoking, resulting in excess survival in HD patients. These findings can help screening programs to identify patients with a high mortality risk.
Acknowledgements
This study is a part of thesis in Ph.D. of Epidemiology at Tehran University of Medical Sciences (Research code: 9221128004). We would like to thank parson participating in this project and the health staff of the hemodialysis wards in hospitals of Hamadan Province for their kind cooperation.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study has been supported by Tehran University of Medical Sciences.
Highlights
-
CRP positive and low level of serum albumin and hemoglobin were associated with increasing death risk in hemodialysis patients.
-
There is a super-additive interaction between CRP status with serum hemoglobin in excess survival of hemodialysis patients.
-
There is a super-additive interaction between CRP status with smoking in excess survival of hemodialysis patients.
References
- Grassmann A, Gioberge S, Moeller S, Brown G. ESRD patients in 2004: global overview of patient numbers, treatment modalities and associated trends. Nephrol Dial Transplant 2005; 20(12):2587-93. [ Google Scholar]
- Collins AJ, Foley RN, Herzog C, Chavers B, Gilbertson D, Ishani A. US renal data system 2010 annual data report. Am J Kidney Dis 2011; 57(Suppl 1):A8, e1-526. [ Google Scholar]
- Mafra D, Farage NE, Azevedo DL, Viana GG, Mattos JP, Velarde LGC. Impact of serum albumin and body-mass index on survival in hemodialysis patients. Int Urol Nephrol 2007; 39(2):619-24. [ Google Scholar]
- Mousavi SSB, Hayati F, Ansari MJA, Valavi E, Cheraghian B, Shahbazian H. Survival at 1, 3, and 5 years in diabetic and nondiabetic patients on hemodialysis. Iran J Kidney Dis 2010; 4(1):74-7. [ Google Scholar]
- Montaseri M, Yazdani Cherat J, Espahbodi F, Mousavi SJ. Five-year survival rate in hemodialysis patients Attending Sari Imam Khomeini Hospital. Journal of Mazandaran University of Medical Sciences 2013; 23(101):78-85. [ Google Scholar]
- Bleyer AJ, Tell GS, Evans GW, Ettinger WH, Burkart JM. Survival of patients undergoing renal replacement therapy in one center with special emphasis on racial differences. Am J Kidney Dis 1996; 28(1):72-81. [ Google Scholar]
- Brodowska-Kania D, Rymarz A, Gibin K. First year survival of patients on maintenance dialysis treatment in Poland. Nagoya J Med Sci 2015; 77(4):629-35. [ Google Scholar]
- Akizawa T, Saito A, Gejyo F, Suzuki M, Nishizawa Y, Tomino Y. Low Hemoglobin Levels and Hypo-Responsiveness to Erythropoiesis-Stimulating Agent Associated With Poor Survival in Incident Japanese Hemodialysis Patients. Ther Apher Dial 2014; 18(5):404-13. [ Google Scholar]
- Iseki K, Tozawa M, Takishita S. Effect of the duration of dialysis on survival in a cohort of chronic haemodialysis patients. Nephrol Dial Transplant 2003; 18(4):782-7. [ Google Scholar]
- VanderWeele TJ, Knol MJ. A tutorial on interaction. Epidemiologic Methods 2014; 3(1):33-72. [ Google Scholar]
- de González AB, Cox DR. Interpretation of interaction: A review. Ann Appl Stat 2007; 1(2):371-85. [ Google Scholar]
- de Mutsert R, Grootendorst DC, Axelsson J, Boeschoten EW, Krediet RT, Dekker FW. Excess mortality due to interaction between protein-energy wasting, inflammation and cardiovascular disease in chronic dialysis patients. Nephrol Dial Transplant 2008; 23(9):2957-64. [ Google Scholar]
- Bottai M, Zhang J. Laplace regression with censored data. Biometrical Journal 2010; 52(4):487-503. [ Google Scholar]
- Bellavia A, Bottai M, Orsini N. Evaluating additive interaction using survival percentiles. Epidemiology 2016; 27(3):360-4. [ Google Scholar]
- Regidor DL, Kopple JD, Kovesdy CP, Kilpatrick RD, McAllister CJ, Aronovitz J. Associations between changes in hemoglobin and administered erythropoiesis-stimulating agent and survival in hemodialysis patients. J Am Soc Nephrol 2006; 17(4):1181-91. [ Google Scholar]
- Gilbertson DT, Ebben JP, Foley RN, Weinhandl ED, Bradbury BD, Collins AJ. Hemoglobin level variability: associations with mortality. Clin J Am Soc Nephrol 2008; 3(1):133-8. [ Google Scholar]
- Furuland H, Linde T, Ahlmén J, Christensson A, Strömbom U, Danielson BG. A randomized controlled trial of haemoglobin normalization with epoetin alfa in pre‐dialysis and dialysis patients. Nephrol Dial Transplant 2003; 18(2):353-61. [ Google Scholar]
- Felker GM, Adams KF, Gattis WA, O'Connor CM. Anemia as a risk factor and therapeutic target in heart failure. J Am Coll Cardiol 2004; 44(5):959-66. [ Google Scholar]
- Dogan E, Erkoc R, Eryonucu B, Sayarlioglu H, Agargun MY. Relation between depression, some laboratory parameters, and quality of life in hemodialysis patients. Ren Fail 2005; 27(6):695-9. [ Google Scholar]
- Collins AJ, Li S, PETER WS, Ebben J, Roberts T, Ma JZ. Death, hospitalization, and economic associations among incident hemodialysis patients with hematocrit values of 36 to 39%. J Am Soc Nephrol 2001; 12(11):2465-73. [ Google Scholar]
- Kalantar-Zadeh K, Supasyndh O, Lehn RS, McAllister CJ, Kopple JD. Normalized protein nitrogen appearance is correlated with hospitalization and mortality in hemodialysis patients with Kt/V greater than 120. J Ren Nutr 2003; 13(1):15-25. [ Google Scholar]
- Kalantar-Zadeh K, Kilpatrick RD, Kuwae N, McAllister CJ, Alcorn H, Kopple JD. Revisiting mortality predictability of serum albumin in the dialysis population: time dependency, longitudinal changes and population-attributable fraction. Nephrol Dial Transplant 2005; 20(9):1880-8. [ Google Scholar]
- Combe C, Chauveau P, Laville M, Fouque D, Azar R, Cano N. Influence of nutritional factors and hemodialysis adequacy on the survival of 1,610 French patients. Am J Kidney Dis 2001; 37(1):S81-S8. [ Google Scholar]
- Mittman N, Avram MM, Oo KK, Chattopadhyay J. Serum prealbumin predicts survival in hemodialysis and peritoneal dialysis: 10 years of prospective observation. Am J Kidney Dis 2001; 38(6):1358-64. [ Google Scholar]
- Yeun JY, Levine RA, Mantadilok V, Kaysen GA. C-reactive protein predicts all-cause and cardiovascular mortality in hemodialysis patients. Am J Kidney Dis 2000; 35(3):469-76. [ Google Scholar]
- Wasserman S, Rosanio S, Tiblier E, Sperger H, Tocchi M, Christenson R. Cardiac troponin T and C-reactive protein for predicting prognosis, coronary atherosclerosis, and cardiomyopathy in patients undergoing long-term hemodialysis. JAMA 2003; 290(3):353-9. [ Google Scholar]
- Lind L. Circulating markers of inflammation and atherosclerosis. Atherosclerosis 2003; 169(2):203-14. [ Google Scholar]
- Kiss I, Kiss Z, Kerkovits L, Paksy A, Ambrus C. Smoking has no impact on survival and it is not associated with ACE gene I/D polymorphism in hemodialysis patients. J Renin Angiotensin Aldosterone Syst 2017; 18(1):1470320316667831. [ Google Scholar]
- Liebman SE, Lamontagne SP, Huang L-S, Messing S, Bushinsky DA. Smoking in dialysis patients: a systematic review and meta-analysis of mortality and cardiovascular morbidity. Am J Kidney Dis 2011; 58(2):257-65. [ Google Scholar]
- Wesson DE, editor. The relationship of cigarette smoking to end-stage renal disease. Seminars in Nephrology; 2003: 23(3): 317-22.
- Orth SR, Hallan SI. Smoking: a risk factor for progression of chronic kidney disease and for cardiovascular morbidity and mortality in renal patients—absence of evidence or evidence of absence?. Clin J Am Soc Nephrol 2008; 3(1):226-36. [ Google Scholar]