J Res Health Sci. 26(1):e00675.
doi: 10.34172/jrhs.11469
Original Article
Trend Analysis of Suicide Mortality and Years of Life Lost from 2012 to 2023 in Khuzestan Province, Iran: A Cross-sectional Study
Habibollah Azarbakhsh Conceptualization, Data curation, Formal analysis, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing, 1 
Seyed Parsa Dehghani Validation, Visualization, Writing – original draft, Writing – review & editing, 2
Elahe Piraie Investigation, Writing – original draft, Writing – review & editing, 3
Mahdiyeh Rashedi Data curation, Project administration, Supervision, Writing – original draft, Writing – review & editing, 4
Reza Davasaz-Irani Project administration, Visualization, Writing – original draft, Writing – review & editing, 4
Fatemeh Rezaei Conceptualization, Methodology, Writing – original draft, Writing – review & editing, 5, *
Author information:
1Social Determinants of Health Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
3Social Determinants of Health Research Center, Yasuj University of Medical Sciences, Yasuj, Iran
4Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
5Research Center for Social Determinants of Health, Jahrom University of Medical Sciences, Jahrom, Iran
Abstract
Background:
The present study was designed to assess the mortality rate and years of life lost due to suicide in Khuzestan province.
Study Design:
A cross-sectional study.
Methods:
In this study, data on all deaths caused by suicide in Khuzestan province were obtained from the population-based Electronic Death Registration System (EDRS). Crude and age-standardized suicide mortality rates (ASR) were calculated based on gender and year of death over the study period. Subsequently, the number of years of life lost (YLL) was calculated based on age and gender. Joinpoint regression analysis was used to examine the trends in crude mortality rates, age-standardized rates (ASRs), and YLL rates.
Results:
During the study years, 1904 suicide deaths occurred in Khuzestan province. Of these deaths, 1157 (60.8%) occurred in men. The highest number of deaths in both genders occurred due to hanging. According to the joinpoint regression, the 12-year trend of YLL rate due to premature mortality was stable. The average annual percentage change (AAPC) was -0.4% (95% CI -4.5 to 7.9, P=0.986) for males, and it was 2.4% (95% CI -1.6 to 7.5, P=0.222) for females. There were 1 joinpoint and 2 time periods for males (2012-2014 (non-significant decreases) and 2014-2023 (significant increases)), and there were 1 joinpoint and 2 time periods for females (2012-2016 (significant decreases) and 2016-2023 (significant increases)).
Conclusion:
The findings revealed a significant increase in age-standardized mortality rate among women and a stable trend among men, and a slight rise in crude mortality rate in men. To address these concerns, it is recommended that targeted region-specific prevention programs be strengthened.
Keywords: Years of life lost, Suicide, Iran, Trend, Mortality rate, Joinpoint regression
Copyright and License Information
© 2026 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Azarbakhsh H, Dehghani SP, Piraie E, Rashedi M, Davasaz-Irani R, Rezaei F. Trend analysis of suicide mortality and years of life lost from 2012 to 2023 in Khuzestan province, Iran: a cross-sectional study. J Res Health Sci. 2026; 26(1):e00675. doi:10.34172/jrhs.11469
Background
According to the definition provided by the World Health Organization (WHO), suicide attempts are actions in which an individual intentionally inflicts harm upon themselves without the interference of others.1 Suicide is considered one of the most significant global public health concerns. It ranks as the 13th leading cause of death overall and the third leading cause of death among individuals aged 15–34 years.2 Approximately 800000 suicide-related deaths occur worldwide annually (one death every 40 seconds).3 Despite a significant decline in the global suicide rate from 13.8% to 9.8% per 100000 people between 1990 and 2019, the overall number of suicide deaths has increased by 19897 cases.4 In 2021, there were 746000 suicide deaths worldwide, 519000 of which occurred in men.The age-standardized mortality rate has declined over time, from 14.9 deaths (12·8–15·7) per 100 000 population in 1990 to 9.0 (8.3–9.6) per 100 000 in 2021.5 This rise imposes significant economic and social costs, resulting in productivity loss and adverse psychological impacts on affected individuals, their social networks, and family members.6 Suicide is a complex and multifactorial phenomenon associated with individual, familial, and social factors, including male gender, younger age, and mental disorders such as schizophrenia.7 The epidemiological distribution of suicide is influenced by a complex interplay of demographic, cultural, economic, and social factors, as well as time, place, accessibility of means, and so on.8 Obtaining accurate data on suicide trends and patterns is challenging, as these data are often underreported due to sociocultural factors.9
Although suicide attempts are generally less prevalent in Islamic countries such as Iran compared to other nations, evidence indicates a rising trend in these regions.10 In Iran, statistics show that between 2006 and 2015, a total of 35279 suicide-related deaths occurred. During this 10-year period, the average total years of life lost (YLLs) due to premature death was 34.52 per 1000 persons in males, 13.61 per 1000 persons in females, and 23.35 per 1000 persons in both genders. The annual change in the YLL rate was reported to be 3.3%.11 The latest reports estimate that the suicide rate in Iran is 6.8 per 100000, which is lower than the global rate and places the country 58th in the world rankings.1 The indicator of YLLs due to premature death is a valuable analytical tool for prioritizing public health concerns. It can be used across different geographic regions by applying time as a measurement unit and comparing years of life lost with the standard life expectancy curve.12 Unlike crude mortality rate, the YLL indicator gives more weight to deaths occurring among young adults.13
Khuzestan province is located in southern Iran and has a population of over 4 million, making it the fifth most populous province in Iran. According to the Statistical Center of Iran, Khuzestan is known as the most emigrant-pole in Iran (according to the last census in 2016). Based on available statistics, more than 50% of them have been rural immigrants.14 Given that no study has been conducted on mortality rates and years of life lost due to suicide in Khuzestan province, the present study was designed to assess the mortality rate and years of life lost due to suicide in Khuzestan province.
Materials and Methods
In this cross-sectional study, data on all deaths caused by suicide in Khuzestan province were obtained from the population-based Electronic Death Registration System (EDRS). Data from health centers and health houses in rural and urban areas, forensic medicine, hospitals, and cemeteries are transmitted to the district health center, where the data is checked with civil registration.15 Therefore, the probability of underreporting the number of suicide cases is minimized. The study period spanned from 2012 to 2023. Extracted variables included age at death, year of death, method of suicide, and gender. Inclusion criteria were residency in Khuzestan province and deaths attributed to intentional self-harm. Causes of death were coded based on the 10th revision of the International Classification of Diseases (ICD-10), specifically codes X60–X84, which pertain to suicide. The total estimated population of Khuzestan province was derived using baseline data from health centers and national census data from 2006 and 2016, adjusted based on annual population growth rates. For standardization, the 2013 WHO standard population for low- and middle-income countries was used.16
Statistical analysis
First, crude and age-standardized suicide mortality rates (ASR) were calculated based on gender and year of death over the study period. Subsequently, the number of YLLs was computed using standard life tables and life expectancy estimates stratified by age and gender, following a specific formula.17 YLL calculations were performed using Microsoft Excel version 2016.
YLL = N Ce(ra) / (β + r)2 [e-(β + r)(L + a) [-(β + r) (L + a)-1] – e-(β + r)a [–(β + r) a-1]]
N represents the number of deaths in each age group and gender. L denotes the standard life expectancy corresponding to that age and gender, and r is the discount rate, set at 0.03. β is the age-weighting parameter, conventionally fixed at 0.04. C is a constant adjustment factor with a value of 0.1658, a indicates the age at death, and e is the base of the natural logarithm, fixed at 2.71.
βdetermines the most valuable ages, and by changing it, the age that yields the most value can be changed. C is an adjustment constant and is chosen so that the age weights do not change the total number of years of life lost. To estimate net present value and years of life lost, the Global Burden of Disease study assumes a 3% discount rate.18
Joinpoint regression analysis was used to examine the trends in crude mortality rates, ASRs, and YLL rates. This method identifies time segments with distinct trends and estimates annual percentage changes (APCs) for each segment based on the slope of the fitted line. Then, the average annual percentage change (AAPC) was calculated to summarize the overall trend.19 This method is a statistical technique used in time series modeling and is widely used in epidemiological studies to model the time trend of incidence and mortality data. It identifies the number (if any) and location of changes in the trend (joinpoints).20 This joinpoint analysis of the trend was carried out by Joinpoint Regression Program version 5.3.0.0.
Results
Mortality rate due to suicide
During the study years, 1904 suicide deaths occurred in Khuzestan province. A total of 1157 deaths (60.8%) occurred in men. The highest number of deaths in both genders was observed in the 15-29 age group (Figure 1). The highest number of deaths in both genders occurred due to hanging. The crude mortality rate in men increased from 11.2 in 2012 to 12.2 in 2023, but it was not statistically significant. AAPC was 0.1% (95% CI -4.5 to 9.0, P = 0.849). The crude mortality rate in women also had a constant trend, 8.6 in 2012 and 8.8 in 2023, and AAPC was 2.4% (95% CI -1.2 to 6.9, P = 0.190) (Table 1, Figure 2). The trend in age-standardized mortality rates has been stable in men but increasing in women. AAPC was 0.7% (95% CI -3.3 to 8.8, P = 0.668) and 3.9% (95% CI 0.9 to 7.2, P = 0.006) for males and females, respectively (Table 1, Figure 3).
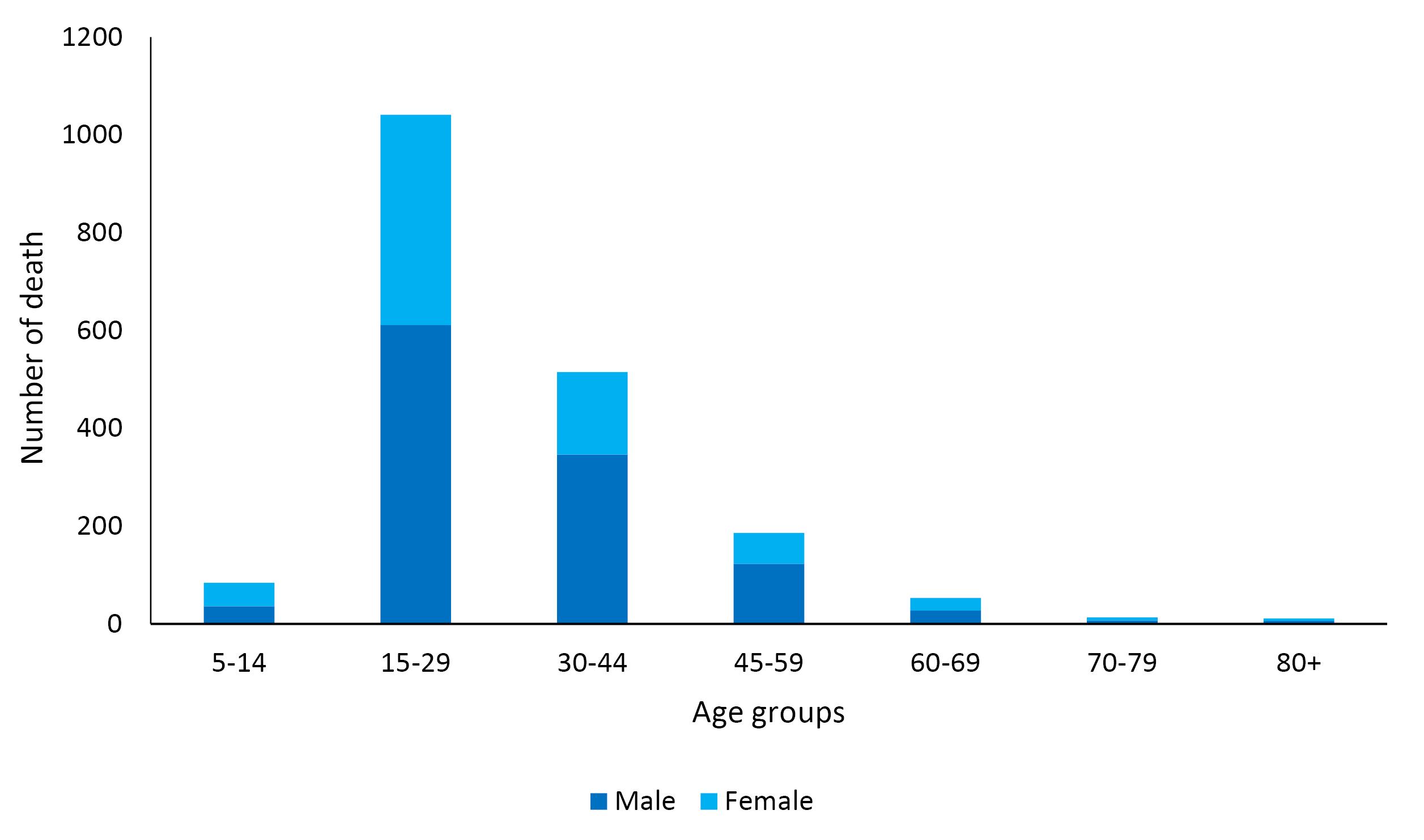
Figure 1.
Number of deaths due to suicide by gender and age groups during 2012-2023
.
Number of deaths due to suicide by gender and age groups during 2012-2023
Table 1.
The Trend of crude and age-standardized mortality rates (per 100000 population) and years of life lost due to suicide by gender and year in Khuzestan province during 2012-2023
|
Year
|
Death (n)
|
Crude mortality rate
|
ASMR (95%CI)
|
Years of life lost
|
|
Death (n)
|
(per 1000)
|
|
Male
|
Female
|
Male
|
Female
|
Male
|
Female
|
Male
|
Female
|
Male
|
Female
|
| 2012 |
134 |
80 |
11.2 |
6.8 |
7.8 (6.3, 9.3) |
4.6 (3.5, 5.8) |
3426 |
2079 |
2.9 |
1.8 |
| 2013 |
88 |
51 |
7.4 |
4.3 |
5.3 (4.1, 6.5) |
3.1 (2.2, 4.1) |
2224 |
1347 |
1.9 |
1.1 |
| 2014 |
45 |
55 |
3.8 |
4.8 |
2.5 (1.6, 3.3) |
3.4 (2.4, 4.3) |
1156 |
1435 |
1.0 |
1.2 |
| 2015 |
74 |
42 |
6.2 |
3.5 |
4.5 (3.4, 5.6) |
2.6 (1.7, 3.4) |
1875 |
1097 |
1.6 |
0.9 |
| 2016 |
56 |
34 |
4.6 |
2.9 |
3.4 (2.4, 4.3) |
2.0 (1.2, 2.7) |
1389 |
933 |
1.2 |
0.8 |
| 2017 |
86 |
49 |
7.1 |
4.1 |
5.0 (3.9, 6.2) |
3.0 (2.1, 3.9) |
2185 |
1291 |
1.8 |
1.1 |
| 2018 |
99 |
50 |
8.1 |
4.2 |
5.8 (4.6, 7.0) |
3.4 (2.5, 4.3) |
2503 |
1283 |
2.0 |
1.1 |
| 2019 |
76 |
69 |
6.1 |
5.7 |
4.4 (3.3, 5.5) |
4.4 (3.2, 5.4) |
1929 |
1788 |
1.6 |
1.5 |
| 2020 |
86 |
53 |
6.9 |
4.3 |
5.4 (4.3, 6.6) |
3.4 (2.5, 4.3) |
2106 |
1369 |
1.7 |
1.1 |
| 2021 |
127 |
78 |
10.1 |
6.3 |
7.5 (6.1, 8.9) |
5.0 (3.9, 6.1) |
3122 |
2081 |
2.5 |
1.7 |
| 2022 |
130 |
75 |
10.2 |
6.0 |
7.3 (5.9, 8.6) |
4.8 (3.7, 5.8) |
3218 |
1895 |
2.5 |
1.5 |
| 2023 |
156 |
111 |
12.2 |
8.8 |
9.4 (8.0, 10.9) |
7.0 (5.7, 8.2) |
3940 |
2867 |
3.1 |
2.3 |
| Total |
1157 |
747 |
7.9 |
5.2 |
5.7 (5.3, 6.1) |
3.9 (3.6, 4.2) |
29073 |
19465 |
2.0 |
1.3 |
|
P-value |
- |
- |
0.849 |
0.190 |
0.668 |
0.006 |
- |
- |
0.986 |
0.222 |
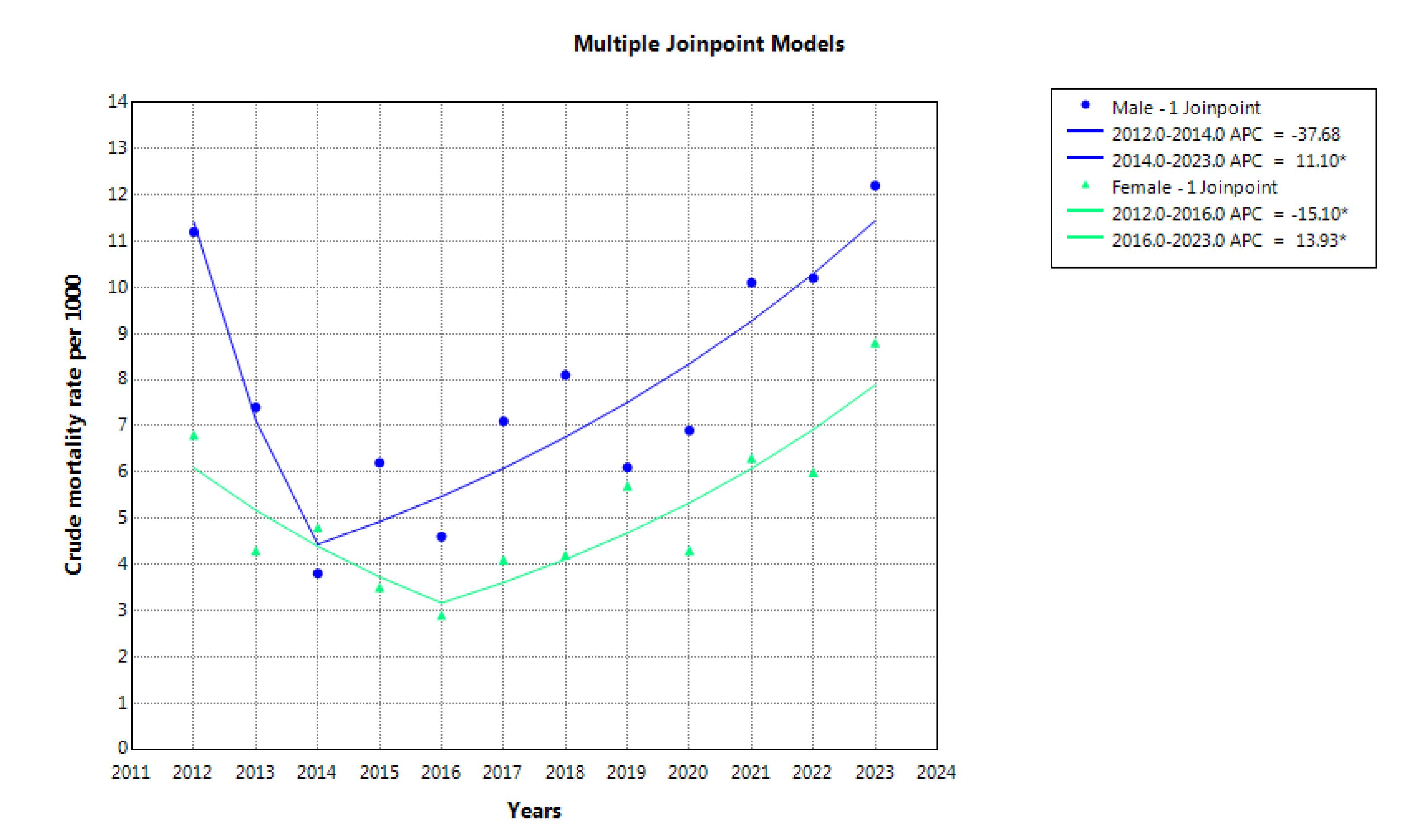
Figure 2.
The trend of crude mortality rate due to suicide in males and females during 2012-2023
.
The trend of crude mortality rate due to suicide in males and females during 2012-2023
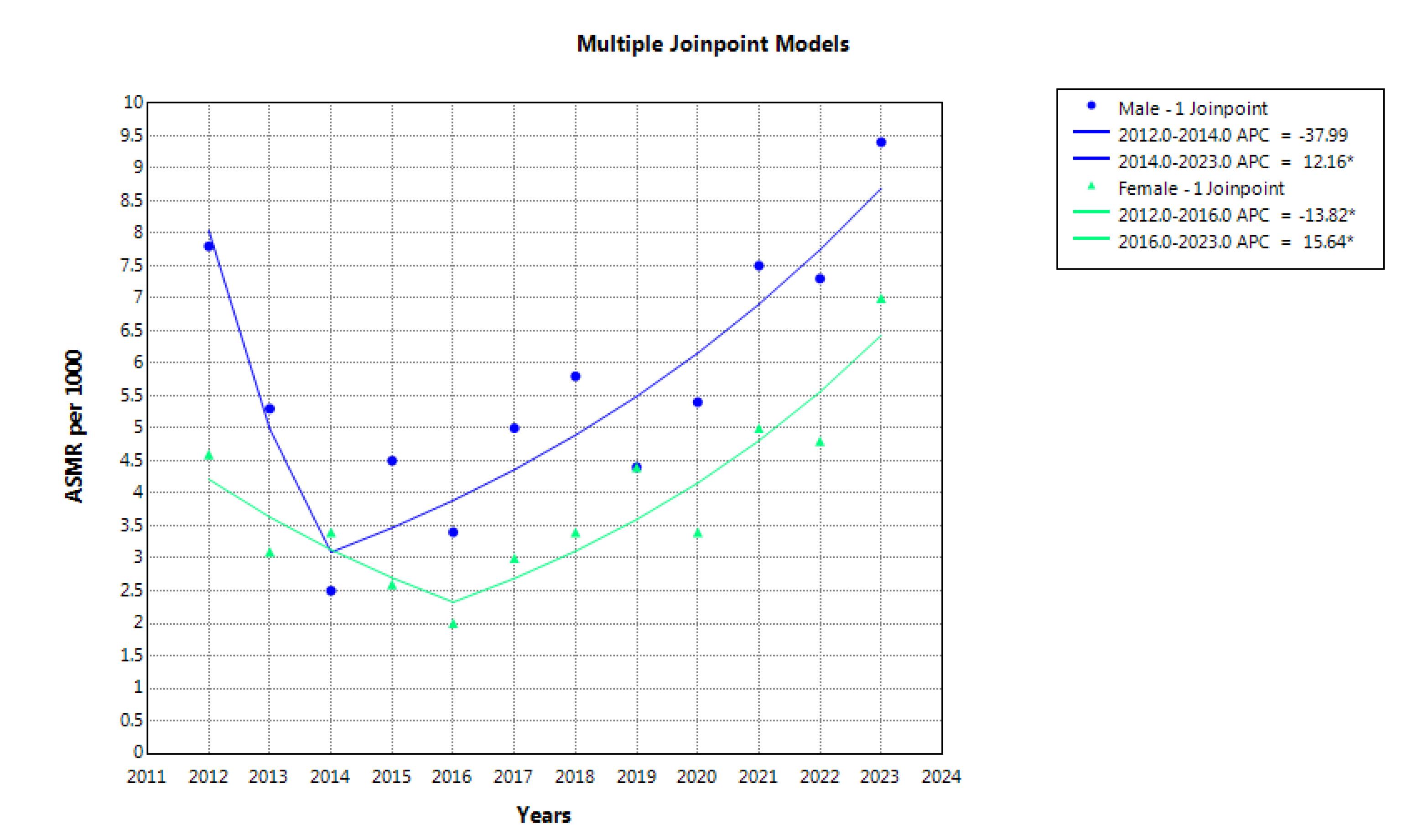
Figure 3.
The trend of age-standardized mortality rate due to suicide in males and females during 2012-2023
.
The trend of age-standardized mortality rate due to suicide in males and females during 2012-2023
YLL due to suicide
The total number of years of life lost due to suicide during the study years was 48538 years, and it was 29073 (59.9%) years in men. The highest number of years of life lost in both genders was attributed to hanging. According to the joinpoint regression, the 12-year trend of YLL rate due to premature mortality was stable. AAPC was -0.4% (95% CI -4.5 to 7.9, P = 0.986) for males, and it was 2.4% (95% CI -1.6 to 7.5, P = 0.222) for females. There were 1 joinpoint and 2 time periods for males. In one period from 2012 to 2014 (the first period), non-significant decreases in YLL rate were seen, and the APC was -37.4% (95% CI -50.6 to 2.3, P = 0.068). In the other period from 2014 to 2023 (the second period), significant increases in YLL rate were seen, and the APC was 10.5% (95% CI 3.3 to 41.8, P = 0.024). There were 1 joinpoint and 2 time periods for females. In one period from 2012 to 2016 (the first period), significant decreases in YLL rate were seen, and the APC was -14.3% (95% CI -36.9 to -0.0, P = 0.050). In the other period from 2016 to 2023 (the second period), significant increases in YLL rate were seen, and the APC was 13.4% (95% CI 6.0 to 43.7, P = 0.006) (Figure 4).
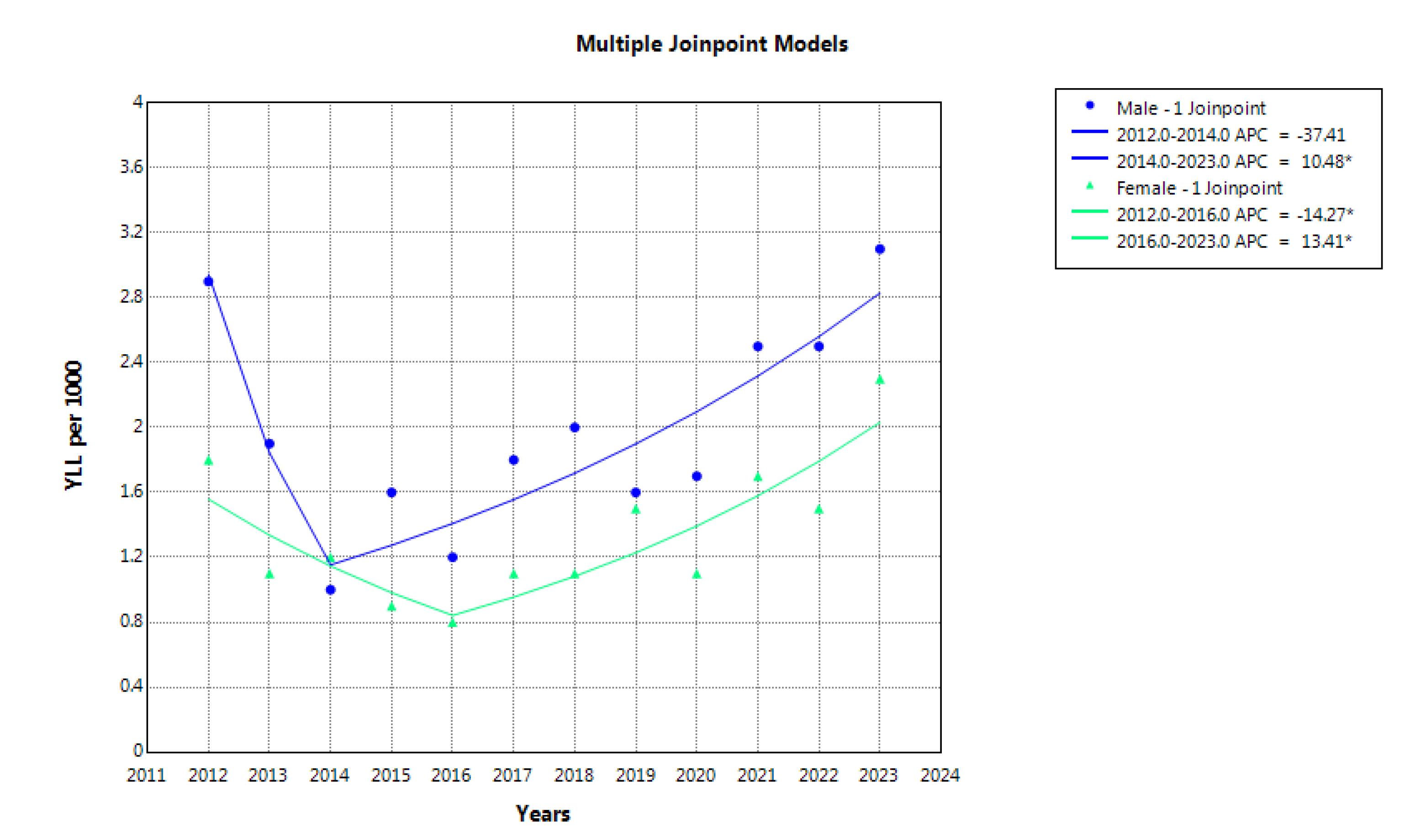
Figure 4.
The trend of years of life lost due to suicide in males and females during 2012-2023
.
The trend of years of life lost due to suicide in males and females during 2012-2023
Discussion
Findings over the 12-year period revealed a slight increase in the crude mortality rate among men, though this change was not statistically significant. Among women, the crude mortality rate remained relatively stable. However, the age-standardized mortality rate (ASMR) showed a significant increase among women, while remaining stable among men. Although the overall YLL trend remained relatively steady, Joinpoint regression analysis revealed two distinct phases: an initial decline followed by a significant increase in YLL rates, beginning in 2014 for men and 2016 for women.
The results showed that over a 12-year period, the crude mortality rate increased from 11.2 to 12.2 per 100000 in men, but it remained almost constant in women. During the same period, age-standardized mortality rates showed a significant increase in women but no significant change in men. The global ASMR due to suicide was estimated to be 9 per 100000 in 2019, with a notably higher rate among men (12.6) compared to women (5.4).21 Reports indicate that the suicide rate in Iran is 6.8 per 100000, ranking 58th globally.22 Notably, the global ASMR has been decreasing.23 Zabihi Afroozi et al found that although suicide attempts were more frequent among women, completed suicides were more common among men, indicating a higher mortality rate due to suicide among males.24 Shakibkhah et al also reported increasing trends in both crude and standardized suicide mortality among men, with stable rates among women.25,26. In a systematic review and meta-analysis, Rouzrokh et al showed that the overall suicide mortality rate was higher among men in Iran, especially non-western men. However, Iranian women in western provinces, especially through self-immolation, showed disproportionately higher suicide rates.26 Similar trends were reported by Park et al in South Korea, indicating increased suicide rates among women over the past decade, attributed in part to rising socio-economic pressures.27 Suicide is a multifactorial phenomenon influenced by cultural, social, and economic factors.26,28 The observed gender differences, particularly the significant increase in female suicide mortality, may be attributed to unique sociocultural structures, lack of social support, domestic violence, the use of violent methods such as self-immolation, entrenched gender biases, restricted freedoms, unemployment, and economic hardship. It is noteworthy that women may encounter unique pressures and challenges that are different from those of men. Women face greater challenges, such as gender-based violence and discrimination in career advancement. In addition, societal and familial expectations to balance career and family responsibilities are among the main challenges women face.29 Therefore, women’s needs should be considered and intervention and educational programs should be implemented to reduce and prevent suicide if necessary. Regional variations may also stem from differences in geography, customs, and lifestyle across Iranian provinces. It is plausible that certain regions harbor specific local risk factors. These findings underscore the need for regionally tailored prevention policies that are sensitive to local cultural and social contexts.
This study confirmed that the highest burden of suicide mortality and YLL occurred among individuals aged 15–29 years, with hanging as the most frequent method of suicide in both genders. These findings align with previous studies conducted in Iran.25 For instance, Shafiee-Kandjani et al reported an overall suicide mortality rate of 8.14 per 100000, with higher rates observed among men (9.1) compared to women (5.0), and hanging as the most common method.30 Similarly, in a multicenter study, Fathi et al highlighted the predominance of youth in suicide-related deaths and confirmed that hanging was the most widespread method across regions.31 There is growing concern about rising suicide rates among Iranian youth, particularly young physicians, which may reflect increasing socio-economic stressors.32 The leading suicide methods vary globally due to differential access to lethal means and cultural-behavioral differences across countries and even within subnational regions.33 Suicide behavior is inherently multifactorial and cannot be attributed to a single determinant. Personality traits may also play a significant role.34. These findings highlight the urgent need for targeted interventions and enhanced mental health infrastructure, particularly for vulnerable youth populations. A better understanding of suicide patterns by age, gender, method, and socioeconomic status can support more effective preventive policies and reduce the public health burden.
Trend analysis of YLL over time is critical for identifying major shifts in population health and guiding policymakers in designing targeted interventions. Joinpoint regression serves as a valuable tool for detecting trend changes and identifying periods of rising or declining YLL rates, thereby enabling timely and appropriate responses.20,35 Our analysis revealed two distinct Joinpoint phases: an initial decline in YLL for both genders, followed by a significant increase from 2014 in men and 2016 in women. These shifts may reflect underlying social, economic, or healthcare-related changes. The early reduction in YLL may be linked to improved healthcare access, increased public awareness, or successful early prevention programs.36 Conversely, the subsequent increase could be attributed to rising psychological and social pressures in Iran and other middle-income countries.37,38 Economic and social stressors likely contributed to higher rates of premature mortality from suicide and psychosomatic diseases, thereby raising overall YLL.23,37 In addition, demographic transitions, such as the rising youth or elderly population, can alter disease burden and influence YLL. A decline in the effectiveness of existing prevention programs may also contribute to this upward trend, suggesting a need for review and recalibration.
Iran’s national suicide prevention program became a part of primary health care in 2010. The goal of this program is to improve suicide prevention efforts across the country.39 However, a national commitment is necessary to decrease the prevalence of suicide through the promotion of good mental health, the reduction of poverty and inequality, the prevention of alcohol and drug use, and the promotion of social justice and human rights.40
The present study has several strengths. First, its longitudinal design over a 12-year period enabled precise identification of temporal changes and turning points in trends. Second, the use of advanced Joinpoint regression analysis offered deeper insights into significant trend shifts, including periods of increase or decline. Third, the application of multidimensional indicators, including crude and age-standardized mortality rates and YLL, provided a comprehensive evaluation of the suicide burden. Nevertheless, several limitations exist. Suicide may be underreported due to social stigma, religious beliefs, and legal implications. The lack of contextual data, such as psychiatric history, socioeconomic status, and access to mental health services, limits our ability to fully understand associated risk factors. Furthermore, given that the study was conducted solely in Khuzestan province, generalizability of the findings to other regions of Iran may be limited due to cultural and economic differences. Finally, reliance on official death registration data may result in the omission of unregistered suicide cases.
Highlights
-
During the study years, 1904 suicide deaths occurred in Khuzestan province.
-
The total YLL due to suicide was 29073 in males and 19465 in females.
-
According to the joinpoint regression analysis, the 12-year trend of YLL rate due to premature mortality was stable.
Conclusion
The findings revealed a significant increase in age-standardized mortality among women, a relatively stable trend among men, and a slight rise in crude mortality in men. The highest burden of suicide mortality and YLL was observed in the 15–29 age group, with hanging identified as the most common suicide method in both genders. Joinpoint regression analysis identified two distinct phases, including an initial decline in YLL followed by a statistically significant increase beginning in 2014 for men and 2016 for women, likely influenced by social, economic, or healthcare dynamics. Since suicide is a multifactorial phenomenon, social, economic, and cultural interventions are needed to prevent and reduce suicide.
Acknowledgments
We would like to acknowledge the Health Vice-chancellor, Ahvaz Jundishapur University of Medical Sciences for providing the resources.
Competing Interests
The authors declare that they have no conflict of interests related to the publication of this study.
Ethical Approval
The protocol of this study was reviewed and approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1402.654). Given the nature of the data and the lack of personal information, there was no need for informed consent. All procedures were conducted in accordance with the ethical code of the university and research standards.
Funding
None.
References
- Asadiyun M, Daliri S. Suicide attempt and suicide death in Iran: a systematic review and meta-analysis study. Iran J Psychiatry 2023; 18(2):191-212. doi: 10.18502/ijps.v18i2.12370 [Crossref] [ Google Scholar]
- Azarbakhsh H, Moftakhar L, Amiri S, Mirahmadizadeh A. Epidemiology of suicide by medication overdose: a population-based study 2011-2019. Arch Med Res 2022; 53(3):304-11. doi: 10.1016/j.arcmed.2021.10.006 [Crossref] [ Google Scholar]
- Azarbakhsh H, Jafari F, Dehghani SP, Hamedi A, Sharifi MH, Mirahmadizadeh A. Trend analysis of suicide and homicide mortality and years of life lost (YLL) in children aged 10-19 years in the south of Iran, 2004-2019. J Res Health Sci 2024; 24(1):e00606. doi: 10.34172/jrhs.2024.141 [Crossref] [ Google Scholar]
- Yan N, Luo Y, Mackay LE, Wang Y, Wang Y, Wang Y. Global patterns and trends of suicide mortality and years of life lost among adolescents and young adults from 1990 to 2021: a systematic analysis for the Global Burden of Disease Study 2021. Epidemiol Psychiatr Sci 2024; 33:e52. doi: 10.1017/s2045796024000532 [Crossref] [ Google Scholar]
- GBD 2021 Suicide Collaborators. Global, regional, and national burden of suicide, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Public Health 2025; 10(3):e189-202. doi: 10.1016/s2468-2667(25)00006-4 [Crossref] [ Google Scholar]
- Rostami M, Jalilian A, Jalilian M, Mahdavi SA. Years of life lost due to complete suicide in Iran: a national registry-based study. J Res Health Sci 2024; 24(1):e00605. doi: 10.34172/jrhs.2024.140 [Crossref] [ Google Scholar]
- Mirahmadizadeh A, Rezaei F, Moftakhar L, Heiran N, Azarbakhsh H. Years of life lost due to suicide in southern Iran 2011-18: a population-based study. Arch Iran Med 2022; 25(1):12-6. doi: 10.34172/aim.2022.03 [Crossref] [ Google Scholar]
- Nazari Kangavari H, Shojaei A, Hashemi Nazari SS. Suicide mortality trends in four provinces of Iran with the highest mortality, from 2006-2016. J Res Health Sci 2017; 17(2):e00382. [ Google Scholar]
- Bertuccio P, Amerio A, Grande E, La Vecchia C, Costanza A, Aguglia A. Global trends in youth suicide from 1990 to 2020: an analysis of data from the WHO mortality database. EClinicalMedicine 2024; 70:102506. doi: 10.1016/j.eclinm.2024.102506 [Crossref] [ Google Scholar]
- Moftakhar L, Mirahmadizadeh A, Amiri S, Rezaei F, Azarbakhsh H. Epidemiology of suicide by hanging in Fars province, Iran (2011-2019): a population-based cross-sectional study. J Prev Med Public Health 2023; 56(3):264-71. doi: 10.3961/jpmph.22.519 [Crossref] [ Google Scholar]
- Izadi N, Mirtorabi SD, Najafi F, Nazparvar B, Nazari Kangavari H, Hashemi Nazari SS. Trend of years of life lost due to suicide in Iran (2006-2015). Int J Public Health 2018; 63(8):993-1000. doi: 10.1007/s00038-018-1151-1 [Crossref] [ Google Scholar]
- Jalilian Z, Mohamadian F, Ahmadi S, Veisani Y. Death trends and years of life lost due to social harms such as suicide, homicide, and addiction, Ilam province, 2009-2019. Bull Emerg Trauma 2023; 11(4):167-72. doi: 10.30476/beat.2023.97876.1447 [Crossref] [ Google Scholar]
- Mirahmadizadeh A, Hassanzadeh J, Janfada M, Azarbakhsh H. The burden of premature mortality in southern Iran during 2004-2019 using standard expected years of life lost: a population-based study. Iran J Public Health 2023; 52(10):2196-206. doi: 10.18502/ijph.v52i10.13858 [Crossref] [ Google Scholar]
- Mohammadi Dehcheshmeh M, Ghaedi S. Climate change and ecological migration: a study of villages in the province of Khuzestan, Iran. Environ Res Eng Manag 2020; 76(1):6-19. doi: 10.5755/j01.erem.76.1.24513 [Crossref] [ Google Scholar]
- Mirahmadizadeh A, Moftakhar L, Dehghani SS, Hassanzadeh J, Dehghani SP, Azarbakhsh H. Mortality rate and years of life lost due to burns in southern Iran during 2004-2019: a population-based study. Arch Iran Med 2023; 26(4):205-11. doi: 10.34172/aim.2023.31 [Crossref] [ Google Scholar]
- Sankoh O, Sharrow D, Herbst K, Whiteson Kabudula C, Alam N, Kant S. The INDEPTH standard population for low- and middle-income countries, 2013. Glob Health Action 2014; 7:23286. doi: 10.3402/gha.v7.23286 [Crossref] [ Google Scholar]
- Azarbakhsh H, Jafari F, Dehghani SP, Karami H, Hassanzadeh J, Mirahmadizadeh A. Trend analysis of deaths with unintentional poisoning and years of life lost in the south of Iran: 2004-2019. J Res Health Sci 2023; 23(3):e00588. doi: 10.34172/jrhs.2023.123 [Crossref] [ Google Scholar]
- Yang BH, Bray FI, Parkin DM, Sellors JW, Zhang ZF. Cervical cancer as a priority for prevention in different world regions: an evaluation using years of life lost. Int J Cancer 2004; 109(3):418-24. doi: 10.1002/ijc.11719 [Crossref] [ Google Scholar]
- Azarbakhsh H, Baeradeh N, Dehghani SP, Hassanzadeh J, Janfada M, Razeghi A. Trend of mortality rate and years of life lost due to cerebrovascular diseases in Fars province, Iran (2004-2019). Arch Iran Med 2023; 26(4):198-204. doi: 10.34172/aim.2023.30 [Crossref] [ Google Scholar]
- Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 2000; 19(3):335-51. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z [Crossref] [ Google Scholar]
- Ilic M, Ilic I. Worldwide suicide mortality trends (2000-2019): a joinpoint regression analysis. World J Psychiatry 2022; 12(8):1044-60. doi: 10.5498/wjp.v12.i8.1044 [Crossref] [ Google Scholar]
- Daliri S, Bazyar J, Sayehmiri K, Delpisheh A, Sayehmiri F. The incidence rates of suicide attempts and successful suicides in seven climatic conditions in Iran from 2001 to 2014: a systematic review and meta-analysis. Sci J Kurdistan Univ Med Sci 2017; 21(6):1-15. doi: 10.22102/21.6.1 [Crossref] [ Google Scholar]
- Naghavi M. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the Global Burden of Disease Study 2016. BMJ 2019; 364:l94. doi: 10.1136/bmj.l94 [Crossref] [ Google Scholar]
- Zabihi Afroozi S, Khafri S, Manouchehri AA, Emami M, Alizadeh H, Moudi S. Epidemiological trend of suicide in north of Iran from 2011 to 2018 with a focus on joinpoint regression. Caspian J Intern Med 2023; 14(2):170-8. doi: 10.22088/cjim.14.2.170 [Crossref] [ Google Scholar]
- Shakibkhah I, Azarbakhsh H, Peyravi M, Ahmadi Marzaleh M, Rafiei Boldaji M. Trend analysis of suicide mortality and years of life lost from 2016 to 2021 in southern Iran. Iran J Public Health 2024; 53(5):1128-36. doi: 10.18502/ijph.v53i5.15594 [Crossref] [ Google Scholar]
- Rouzrokh P, Abbasi Feijani F, Moshiri Y, Ghahramani S, Bagheri Lankarani K. The pooled prevalence of attributed factors of suicide in Iran: a systematic review and meta-analysis. Arch Iran Med 2025; 28(1):44-60. doi: 10.34172/aim.31276 [Crossref] [ Google Scholar]
- Park S. Brief report: Sex differences in suicide rates and suicide methods among adolescents in South Korea, Japan, Finland, and the US. J Adolesc 2015; 40:74-7. doi: 10.1016/j.adolescence.2015.01.007 [Crossref] [ Google Scholar]
- Hee Ahn M, Park S, Ha K, Choi SH, Hong JP. Gender ratio comparisons of the suicide rates and methods in Korea, Japan, Australia, and the United States. J Affect Disord 2012; 142(1-3):161-5. doi: 10.1016/j.jad.2012.05.008 [Crossref] [ Google Scholar]
- Richardson C, Robb KA, McManus S, O’Connor RC. Psychosocial factors that distinguish between men and women who have suicidal thoughts and attempt suicide: findings from a national probability sample of adults. Psychol Med 2023; 53(7):3133-41. doi: 10.1017/s0033291721005195 [Crossref] [ Google Scholar]
- Shafiee-Kandjani AR, Azizi H, Malek A, Aslrahimi V, Hassanpour M, Kalejahi P. Epidemiology and predictors of suicide and suicide attempt in northwest Iran: a pilot study for local prevention strategies. Sci Rep 2025; 15(1):14734. doi: 10.1038/s41598-025-99895-9 [Crossref] [ Google Scholar]
- Fathi M, Malakouti SK, Rezaeian M, Sayehmiri K, Sheikhtaheri A, Ghaemmaghamfarahani I. A multicenter registry experience for suicidal behaviors in Iran (2019-2022). Arch Iran Med 2024; 27(7):371-8. doi: 10.34172/aim.28558 [Crossref] [ Google Scholar]
- Gharaati Jahromi MS. Burnout, suicide, and emigration: why so many Iranian doctors consider quitting medicine. BMJ 2025; 389:r655. doi: 10.1136/bmj.r655 [Crossref] [ Google Scholar]
- Veisani Y, Delpisheh A, Mohamadian F, Valizadeh R. Trends of suicide attempts and completed suicide in Ilam province of Iran; a demographic analysis study. Bull Emerg Trauma 2018; 6(3):245-8. doi: 10.29252/beat-0603010 [Crossref] [ Google Scholar]
- Azizpour Y, Sayehmiri K, Asadollahi K, Kaikhavani S, Bagheri M. Epidemiological study of suicide by physical methods between 1993 and 2013 in Ilam province, Iran. BMC Psychiatry 2017; 17(1):304. doi: 10.1186/s12888-017-1461-5 [Crossref] [ Google Scholar]
- Balooch Hasankhani M, Haghdoost A, Jahani Y. The concept and application of the joinpoint regression model in analyzing the time trend in epidemiological studies (case: liver cancer due to alcohol use in Iran). Iran J Epidemiol 2023; 19(2):133-42. [ Google Scholar]
- Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet 2017; 389(10075):1229-37. doi: 10.1016/s0140-6736(16)32380-7 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Drinking-Water. 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/drinking-water.
- Reeves A, McKee M, Stuckler D. Economic suicides in the great recession in Europe and North America. Br J Psychiatry 2014; 205(3):246-7. doi: 10.1192/bjp.bp.114.144766 [Crossref] [ Google Scholar]
- Rezaeian M, Platt S, Arensman E. Iran’s national suicide prevention program. Crisis 2022; 43(4):344-7. doi: 10.1027/0227-5910/a000788 [Crossref] [ Google Scholar]
- Rezaeian M. Islam and suicide: a short personal communication. Omega (Westport) 2008; 58(1):77-85. doi: 10.2190/om.58.1.e [Crossref] [ Google Scholar]