J Res Health Sci. 23(4):e00593.
doi: 10.34172/jrhs.2023.128
Review Article
Comparing the Efficacy and Adverse Events of Available COVID-19 Vaccines Through Randomized Controlled Trials: Updated Systematic Review and Network Meta-analysis
Shima Hossaini 1  , Fariba Keramat 2, Zahra Cheraghi 1, 3, Bushra Zareie 1, Amin Doosti-Irani 1, 4, *
, Fariba Keramat 2, Zahra Cheraghi 1, 3, Bushra Zareie 1, Amin Doosti-Irani 1, 4, *
Author information:
1Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Infectious Disease, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
3Modeling of Noncommunicable Diseases Research Center, Hamadan University of Medical Sciences, Hamedan, Iran
4Research Center for Health Sciences, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: Different vaccines have so far been developed and approved to cope with COVID-19 in the world. The aim of this updated network meta-analysis (NMA) was to compare and rank all available vaccines in terms of efficacy and complications simultaneously.
Study Design: A systematic review.
Methods: Three major international databases, including Web of Science, Medline via PubMed, and Scopus, were searched through September 2023. The transitivity assumption was evaluated qualitatively in terms of epidemiologic effect modifiers. The exposure of interest in this study was receiving any available COVID-19 vaccine, and the primary outcome of interest was the incidence of symptomatic COVID-19. In this NMA, the relative risk of symptomatic COVID-19 was used to summarize the efficacy of vaccines in preventing COVID-19. The data were analyzed using the frequentist-based approach, and the results were reported using a random-effects model. Finally, the vaccines were ranked using a P-score.
Results: In total, 34 randomized controlled trials (RCTs) met the eligibility criteria for this systematic review and NMA out of 3682 retrieved references. Based on the results of the NMA, mRNA-1273 was the most effective vaccine in preventing COVID-19 and demonstrated the highest P-score (0.93). The relative risk (RR) for mRNA-1273 versus placebo was 0.07 (95% confidence interval [CI]: 0.03, 0.17). The second and third-ranked vaccines were BNT-162b2 (RR=0.08; 95% CI: 0.04, 0.15; P-score=0.93) and Gam-COVID-Vac (0.09; 95% CI: 0.03, 0.25; 0.88).
Conclusion: Based on the results of this NMA, it seems that all available vaccines were effective in COVID-19 prevention. However, the top three ranked vaccines were mRNA-1273, BNT-162b2, and Gam-COVID-Vac, respectively.
Keywords: COVID-19 Vaccines, Vaccine efficacy, Network meta-analysis
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Hossaini S, Keramat F, Cheraghi Z, Zareie B, Doosti Irani A. Comparing the efficacy and adverse events of available COVID-19 vaccines through randomized controlled trials: updated systematic review and network meta-analysis. J Res Health Sci. 2023; 23(4):e00593. doi:10.34172/jrhs.2023.128
Background
In the COVID-19 pandemic, providing an effective vaccine was one of the main concerns of health policymakers and scientists. Consequently, different vaccines have been developed and approved to cope with this disease around the world. As of July 10, 2023, a total of almost 13.500 billion vaccine doses had been administered worldwide. As of July 19, 2023, the reported confirmed cases of COVID-19 and the deaths due to this disease were over nearly 750 million and nearly seven million, respectively.1 Although the COVID-19 pandemic has subsided, this disease still exists in the world, and there is a risk of future epidemics; thus, countries should be ready to combat it. Vaccination is one of the most effective strategies for preventing infectious diseases.
The available vaccines include DNA, mRNA, vector, protein subunit, inactivated virus, live attenuated, and non-replicating viral vector vaccines.2 Although all available vaccines are effective in preventing COVID-193 selecting the best vaccine among the available vaccines is a main challenge for health policymakers. The first approved vaccine against the COVID-19 virus was Pfizer. The efficacy of this vaccine in phase 3 randomized controlled trials (RCTs) with over 40,000 participants was 91.3%.4 After Pfizer, other countries and companies developed other vaccines. The Sinovac, AstraZeneca, Russian Sputnik, Johnson & Johnson, and Moderna vaccines have an efficacy of 51%,5 63%,6 97.6%,7 66.9%,8 and 93.2%,9 respectively. In addition, the efficacy of Soberana 02 and Soberana Plus vaccines is 49.7 and 64.9%,10 respectively.
In most phase 3 RCTs, all the vaccines have been compared with a placebo, so the safety, efficacy, and complications of the vaccines have been compared directly with a placebo, but a major question is regarding the simultaneous comparisons of all the available vaccines in terms of safety, efficacy, and complications two by two. It would be ideal if we had access to an RCT comparing all vaccines simultaneously, but there are no such RCTs. In the absence of such trials, indirect comparison via network meta-analysis (NMA) may be useful for simultaneous comparison.
To date, there have been a few NMAs that have compared vaccines simultaneously. In an NMA that compared nine vaccines, BNT162b2, mRNA-1273, and Gam-COVID-Vac were the top three vaccines in terms of efficacy.11 Based on the results of a systematic review and NMA of 35 trials, the mRNA vaccines were most effective in preventing COVID-19.3 In an NMA comparing 16 vaccines for efficacy based on the results of this study, BNT126b2, mRNA-1273, and rAd26 & rAd5 vaccines were the top three vaccines.12 Based on the results of another NMA comparing 28 vaccines, the Pfizer vaccine was the most effective in preventing severe COVID-19 infection.13 Although there are some published NMAs,12-14 the vaccines included in these NMAs are not all ones that are available now because the results of some of the phase 3 trials have not been published. Accordingly, the aim of this updated NMA was to compare and rank all available vaccines with published results of phase 3 trials in terms of efficacy and complications simultaneously.
Methods
This NMA is part of a comprehensive systematic review that has simultaneously compared all available vaccines for safety, immunogenicity, efficacy, and related complications in phase 1, 2, and 3 RCTs. In this NMA, we analyzed only the results of phase 3 RCTs. In this systematic review and NMA, we followed the PRISMA guidelines for NMA.15 The efficacy of the vaccine is the performance of a vaccine under idealized conditions of an RCT.16
Search Strategy
A search strategy was developed to identify all pertinent RCTs. Our search strategy is presented in Table S1 (see Supplementary file 1). Three major international databases, including Web of Science, Scopus, and Medline via PubMed, were searched through September 2023. We set up alerts in these databases and continued updating our search until the time of analysis.
Eligibility Criteria and Study Selection
All phase 3 RCTs comparing COVID-19 vaccines with either a placebo or another vaccine were included regardless of study location, population, or language. The phase 1, 2, and 4 studies and non-randomized trials were excluded from this NMA.
Two authors (Sh. H.) and (B. Z.) were responsible for screening the results of our search. All retrieved studies were imported into EndNote software (version X7), and duplicate studies were identified by software and manual review and finally excluded from the pool of studies. Next, the two authors mentioned above independently screened the studies based on their titles and abstracts. Any disagreement between the two authors was resolved by discussion and the judgment of the third reviewer (A. D. I.). Finally, the full texts of selected RCTs were screened according to the mentioned inclusion criteria, and eligible RCTs were identified for data extraction.
The study’s primary and secondary outcomes included the frequency of symptomatic COVID-19 infection and vaccine complications such as localized reactions, fatigue, chills, fever, pain, and headache.
Data Extraction
The eligible RCTs were analyzed, with data extracted on the characteristics of the RCTs, such as the first author’s name, publication year, country, study population, duration of follow-up, data-analysis approach (intention to treat or per protocol), and sample size; the other obtained data were vaccine data (i.e., the exact type of vaccine used in each RCT), potential effect modifiers (e.g., gender and age of participants), and outcomes (i.e., the number of confirmed COVID-19 cases in the vaccine and placebo groups, and efficacy with a 95% confidence interval [CI]), and any reported adverse events in the vaccine and placebo groups.
Risk of Bias Assessment
The Cochrane tool was used to assess the risk of bias.17 Two authors (Sh. H. and A. D. I.) were responsible for the risk of bias assessment. Several items from this tool were used, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. The included RCTs were classified as low, high, moderate, and risk of bias if all items were met, if one item was not met, and if more than one item was not met, respectively.17 Review Manager 5.4 was utilized to assess the risk of bias.18
Data Analysis
The transitivity assumption was evaluated qualitatively in terms of epidemiologic effect modifiers. In this NMA, age and the study population were considered the main effect modifiers. The heterogeneity of pairwise comparisons and the network was assessed using the χ2 test and the I2 statistic. The restricted maximum likelihood estimator was used to calculate the between-study variance.19 The consistency assumption was not assessed in this NMA because there was no closed loop in our networks.20 The available vaccines were presented through a network diagram. The study employed relative risk (RR) to summarize their efficacy in preventing COVID-19 in the NMA. The obtained data were analyzed using the frequentist-based approach, and the results were reported by a random-effects model.
Eventually, the vaccines were ranked using a P-score. The value of the P-score is between zero and one, and a higher value of the P-score indicates a better rank for a vaccine. The P-score for each vaccine is calculated using the one-sided P-value of rejecting the null hypothesis (Pj). In a network, the P-score for each treatment is the mean of all 1-P[j].21 Publication bias was evaluated visually using an adjusted network funnel plot and Egger test.22 The results were reported with a 95% CI. Statistical analysis was conducted using R version 4.0.0 (2020-04-24), and the “netmeta” package was used for NMA.
Results
Overall, 34 RCTs4-7,9,10,23-50 met the eligibility criteria for this systematic review and NMA out of 3682 retrieved references (Figure 1). Of these studies, 26, 5, and 2 RCTs were conducted only on adults of both genders, only on children, on people aged 50 years and older, respectively, and one study was performed on both adults and children. Based on our assessment of the transitivity assumption, the included RCTs were divided into those conducted on adults, children, and the elderly. The results of the risk of bias assessment are shown in Figure 2. The characteristics of the included RCTs are provided in Table 1.
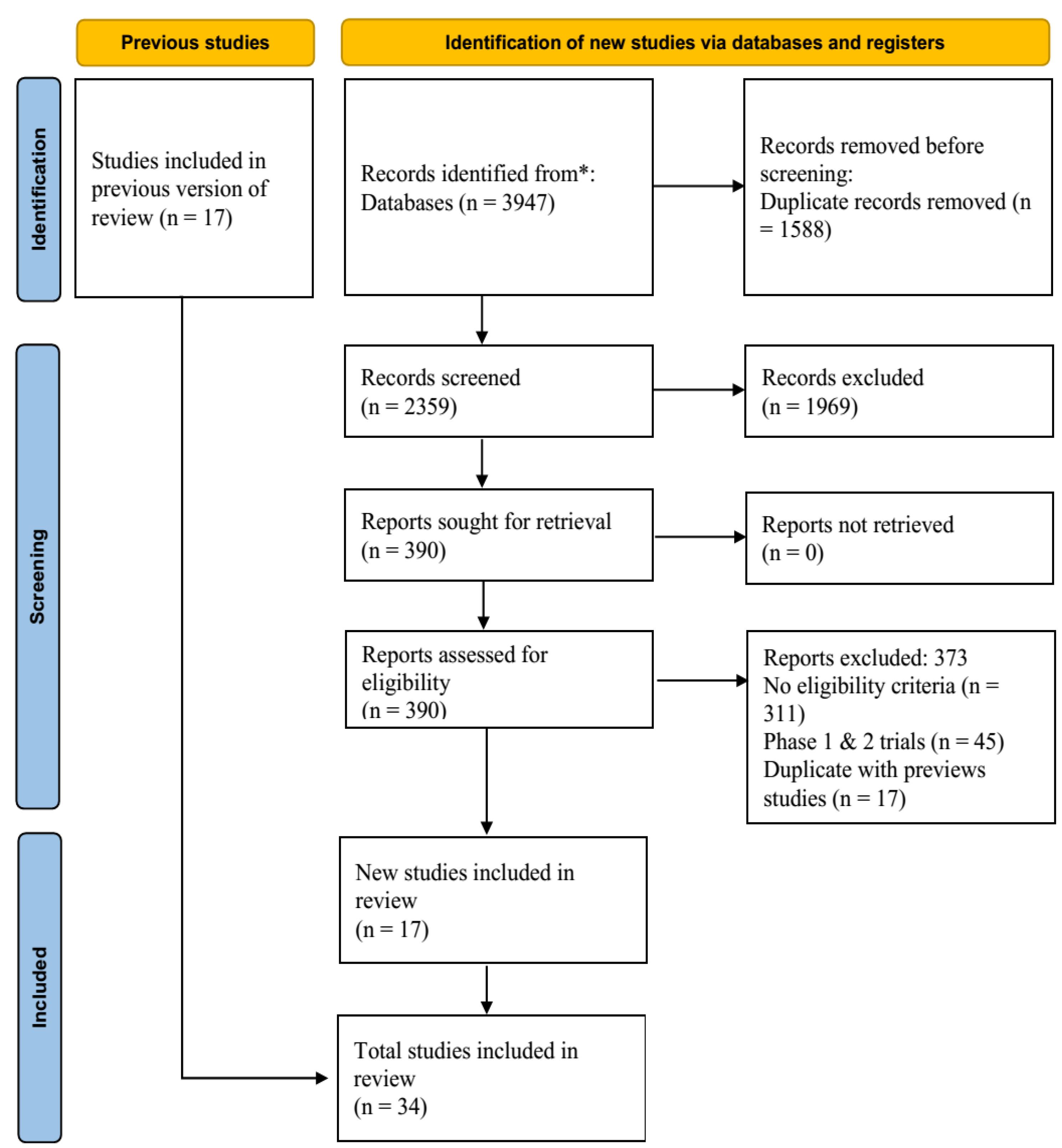
Figure 1.
The flow diagram for the process of study identification for network meta-analysis
.
The flow diagram for the process of study identification for network meta-analysis
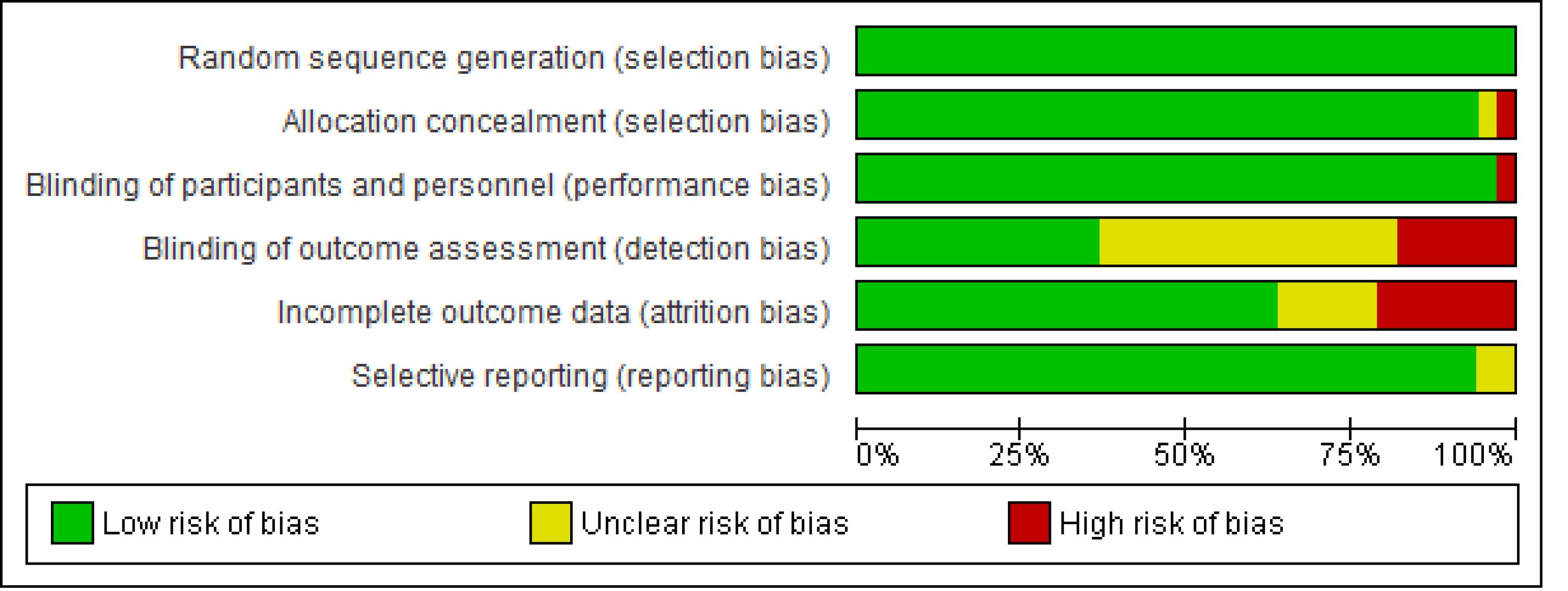
Figure 2.
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies
.
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies
Table 1.
Characteristics of the included randomized controlled trials in the study
|
Author (y)
|
Country
|
Study population
|
Sample size
|
Mean age (y)
|
Male proportion (%)
|
Median duration of follow-up (days)
|
Analysis
|
Loss to Follow-up (%)
|
Vaccines/Placebo
|
Confirmed Cases of COVID-19
|
Efficacy (95% CI)
|
| Polack (2020) 4 |
International |
Healthy adults |
total: 43548
n1: 18860
n2: 18846 |
Arm1: 52
Arm2: 52 |
Arm1:51.1
Arm2: 50.1 |
60 |
ITT |
Arm1: 1.6
Arm2: 1.7 |
Arm1: BNT162b2(30µg)
Arm2: Placebo |
Arm1: 9
Arm2: 169 |
94.6 (89.9, 97.3) |
| Tanriover (2021) 5 |
Turkey |
Healthy adults |
total: 10218
n1: 6650
n2: 3568 |
Arm1: 45
Arm2: 45 |
Arm1:57.4
Arm2: |
43 |
ITT |
Arm1: 1.4
Arm2: 2.7 |
Arm1: CoronaVac
Arm2: Placebo |
Arm1:9
Arm2: 32 |
83.5 (65.4, 92.1) |
| Emary (2021) 6 |
UK |
Healthy adults |
total: 8534
n1: 4244
n2: 4290 |
Arm1: 45
Arm2: 45 |
Arm1:41.4
Arm2: 39.9 |
48 |
Interim analysis |
Arm1: 32.0
Arm2: 21.5 |
Arm1: ChAdOx1 nCoV-19
Arm2: MenACWY |
Arm1:59
Arm2: 210 |
72.3 (63.1, 79.3) |
| Logunov (2021) 7 |
Russia |
Healthy adults |
total: 21977
n1: 16501
n2: 5476 |
Arm1: 45.3
Arm2: 45.3 |
Arm1:55.4
Arm2: 55.1 |
48 |
PP |
Arm1: 0.4
Arm2: 0.7 |
Arm1: Gam-COVID-Vac
Arm2: Placebo |
Arm1:13
Arm2: 47 |
91.1 (83.8, 95.1) |
| Baden (2021) 9 |
USA |
Healthy adults |
total: 30415
n1: 15209
n2: 15206 |
Arm1: 51.4
Arm2: 51.3 |
Arm1:52.1
Arm2: 53.0 |
60 |
ITT* |
Arm1: 3.0
Arm2: 3.0 |
Arm1: mRNA-1273(100µg)
Arm2: Placebo |
Arm1:55
Arm2: 751 |
93.2 (91.1, 94.9) |
| Mostafavi (2023) 10 |
Iran |
Healthy adults |
total: 18000
n1: 14375
n2: 3597 |
Arm1: 39.4
Arm2: 39.1 |
Arm1:60.1
Arm2: 59.1 |
100 |
ITT |
Arm1: 3.7
Arm2: 4.0 |
Arm1: FINLAY-FR-2 (25 μg)
Arm2: Placebo |
Arm1:461
Arm2: 221 |
49.7 (40.8, 57.3) |
| Mostafavi (2023) 10 |
Iran |
Healthy adults |
total: 6000
n1: 4790
n2: 1197 |
Arm1: 39.6
Arm2: 39.9 |
Arm1:59.8
Arm2: 59.9 |
142 |
ITT |
Arm1: 12.8
Arm2: 13.2 |
Arm1: FINLAY-FR-2(25 μg) + FINLAY-FR-1A (50 μg)
Arm2: Placebo |
Arm1:75
Arm2: 51 |
64.9 (49.7, 59.5) |
| Kaabi (2021)23 |
UAE |
Healthy adults |
total: 40411
n1: 13066
n2: 13068
n3: 13071 |
Arm1: 36.2
Arm2: 36.1
Arm3: 36.1 |
Arm1: 81.9
Arm2: 82.3
Arm3: 82.7 |
77 |
PP* |
Arm1: 3.0
Arm2: 2.9
Arm2: 3.0 |
Arm1: SARS-CoV-2 WIV04 (0.5 µg)
Arm2: HB02 (4 µg)
Arm3: Alum |
Arm1: 26
Arm2: 21
Arm3: 95 |
72.8 (58.1, 82.4)
78.1 (64.8, 86.3) |
| Ali (2021) 24 |
USA |
Young adults |
total: 3732
n1: 2489
n2: 1243 |
Arm1: 14.3
Arm2: 14.2 |
Arm1:51.5
Arm2: 50.8 |
83 |
PP |
Arm1: 2.5
Arm2: 16.6 |
Arm1: mRNA-1273 (100 µg)
Arm2: Placebo |
Arm1:1
Arm2: 7 |
93.3 (47.9, 99.9) |
| Bravo (2022) 25 |
Belgium & … |
Healthy adults |
total: 30174
n1: 15092
n2: 15082 |
Arm1: 31.2
Arm2: 31 |
Arm1:22.5
Arm2: 22.5 |
60 |
PP |
Arm1: 58.4
Arm2: 59.4 |
Arm1: SCB-2019 (30 µg)
Arm2: Placebo |
Arm1:63
Arm2: 185 |
67.2 (54.3, 76.8) |
| C.B. Creech (2022) 26 |
USA |
Children |
total: 4016
n1: 3012
n2: 1004 |
Arm1: 8.5
Arm2: 8.5 |
Arm1:51.6
Arm2: 47.9 |
82 |
PP |
Arm1: 1.6
Arm2: 14.6 |
Arm1: mRNA-1273 (50 µg)
Arm2: Placebo |
Arm1:3
Arm2: 4 |
88.0 (70.0, 95.8) |
| Dai (2020) 27 |
Asia |
Healthy adults |
total: 28904
n1: 14453
n2: 14451 |
Arm1: 52
Arm2: 52 |
Arm1:51.1
Arm2: 50.1 |
50.4 |
ITT |
Arm1: 1.6
Arm2: 1.7 |
Arm1: ZF2001
Arm2: Placebo |
Arm1: 36
Arm2: 188 |
81.4 (73.3, 87.3) |
| L.M. Dunkle (2022) 28 |
USA |
Healthy adults |
total: 29949
n1: 19965
n2: 9984 |
Arm1: 47
Arm2: 47 |
Arm1:45.3
Arm2: 41.4 |
60 |
PP |
Arm1: 13.3
Arm2: 18.5 |
Arm1: NVX-CoV2373
Arm2: Placebo |
Arm1:14
Arm2: 63 |
90.4 (82.9, 94.6) |
| Ella (2021) 29 |
India |
Healthy adults |
total: 25798
n1: 12899
n2: 12899 |
Arm1: 40.1
Arm2: 40.1 |
Arm1:67.2
Arm2: 66.8 |
146 |
PP |
Arm1: 6.9
Arm2: 6.9 |
Arm1: BBV152
Arm2: Placebo |
Arm1: 24
Arm2: 106 |
77.8 (65.2, 86.4) |
| Fadlyana (2021) 30 |
Indonesia |
Healthy adults |
total: 1819
n1: 811
n2: 809 |
Arm1: 35.6
Arm2: 35.4 |
Arm1:62.3
Arm2: 66.9 |
90 |
ITT |
Arm1: 1.5
Arm2: 0.7 |
Arm1: Sinovac
Arm2: Placebo |
Arm1:7
Arm2: 18 |
65.3 |
| Falsey (2021) 31 |
USA |
Healthy adults |
total: 63171
n1: 42352
n2: 20747 |
Arm1: 50.2
Arm2: 50.2 |
Arm1:28.4
Arm2: 28.9 |
61 |
ITT |
Arm1: 1.5
Arm2: 2.4 |
Arm1: ChAdOx1 nCoV-19
Arm2: Placebo |
Arm1:168
Arm2: 214 |
74.0 (65.5, 80.5) |
| Frenck Jr. (2021) 32 |
USA |
Healthy adults |
total: 2264
n1: 1134
n2: 1130 |
Arm1: 13.6
Arm2: 13.6 |
Arm1:50.0
Arm2: 51.8 |
60 |
ITT |
Arm1: 1.4
Arm2: 2.5 |
Arm1: BNT162b2
Arm2: Placebo |
Arm1:0
Arm2: 16 |
100 (75.3, 100.0) |
| Frenck Jr. (2021) 32 |
USA |
Children |
total: 3788
n1: 1875
n2: 1913 |
Arm1: 19.4
Arm2: 19.6 |
Arm1:13.6
Arm2: 14.1 |
60 |
ITT |
Arm1: 3.8
Arm2: 5.5 |
Arm1: BNT162b2
Arm2: Placebo |
Arm1: NR
Arm2: NR |
100.0 |
| B. Gilbert (2022) 33 |
USA |
Healthy adults |
total: 1147
n1: 1010
n2: 137 |
Arm1: NR
Arm2: NR |
Arm1:NR
Arm2: NR |
116 |
PP |
Arm1: NR
Arm2: NR |
Arm1: mRNA-1273
Arm2: Placebo |
Arm1:NR
Arm2: NR |
78.0 (54.0, 89.0) |
| Halperin (2022) 34 |
Chile & … |
Healthy adults |
total 36982
n1: 18493
n2: 18489 |
Arm1: 37.8
Arm2: 37.7 |
Arm1:40.3
Arm2: 41.0 |
45 |
ITT |
Arm1: 2.6
Arm2: 2.5 |
Arm1: Ad5-nCoV
Arm2: Placebo |
Arm1:45
Arm2: 105 |
57.5 (39.7, 70.0) |
| Hardt (2022) 35 |
International |
Healthy adults |
total: 31300
n1: 15708
n2: 15592 |
Arm1: 53
Arm2: 53 |
Arm1:52.9
Arm2: 52.3 |
70 |
PP |
Arm1: 52.4
Arm2: 55.1 |
Arm1: Ad26.COV2.S
Arm2: Placebo |
Arm1:14
Arm2: 53 |
75.6 (55.5, 87.5) |
| Heath (2023) 36 |
United Kingdom |
Healthy adults |
total: 15185
n1: 7569
n2: 7569 |
Arm1: 53.4
Arm2: 53.4 |
Arm1:47.5
Arm2: 47.8 |
135 |
ITT |
Arm1: 0.0
Arm2: 0.0 |
Arm1:NVX-CoV2373
Arm2: Placebo |
Arm1:134
Arm2: 24 |
68.7 (58.1, 76.6) |
| Khairullin (2022) 37 |
Kazakhstan |
Healthy adults |
total: 3000
n1: 2400
n2: 600 |
Arm1: 35
Arm2: 34 |
Arm1:50.2
Arm2: 52.2 |
180 |
ITT |
Arm1: 3.0
Arm2: 2.7 |
Arm1:QazCovid-in(5µg)
Arm2: Placebo |
Arm1:31
Arm2: 43 |
82 (71.1, 88.5) |
| Khobragade (2022) 38 |
India |
Healthy adults |
total: 27703
n1: 13851
n2: 13852 |
Arm1: 36.4
Arm2: 36.6 |
Arm1:67.5
Arm2: |
350 |
PP |
Arm1: 1.5
Arm2: 1.6 |
Arm1:ZyCoV-D(2mg)
Arm2: Placebo |
Arm1:20
Arm2: 61 |
66.6 (47.6, 80.7) |
| Kremsner (2022) 39 |
10 countries |
Healthy adults |
total: 39680
n1: 19846
n2: 19834 |
Arm1: 43
Arm2: 43 |
Arm1:54.7
Arm2: 54.5 |
48.2 |
ITT |
Arm1: 2.1
Arm2: 6.8 |
Arm1:CVnCoV
Arm2: Placebo |
Arm1:83
Arm2: 145 |
70.7(42.5, 86.1) |
| Lioznov (2023) 40 |
Russia |
Healthy adults |
total: 783
n1: 374
n2: 126 |
Arm1: 41.2
Arm2: 41 |
Arm1:40.4
Arm2: 38.1 |
210 |
PP |
Arm1: 3.5
Arm2: 4.8 |
Arm1: Ad5-nCoV(0·5mL)
Arm2: Placebo |
Arm1:18
Arm2: 13 |
NR |
| Moreira (2022) 41 |
USA |
Healthy adults |
total:10136
n1: 5088
n2: 5048 |
Arm1: 51.8
Arm2: 51.7 |
Arm1:48.3
Arm2: 49.9 |
75 |
interim analysis |
Arm1: 0.2
Arm2: 0.9 |
Arm1:BNT162b2(30µg)
Arm2: Placebo |
Arm1:15
Arm2: 141 |
89.8 (82.6, 94.4) |
| F.M. Muñoz (2023) 42 |
|
Children 6 Months to < 2 Y |
total: 1776
n1: 1178
n2: 598 |
Arm1: 1.26
Arm2: 1.28 |
Arm1:50
Arm2: |
40 |
ITT |
Arm1: 0.8
Arm2: 0.7 |
Arm1:BNT162b2(3µg)
Arm2: Placebo |
Arm1:4
Arm2: 8 |
75.8 (9.7, 94.7) |
| F.M. Muñoz (2023) 42 |
|
Children 2 to 4 Yr |
total: 2750
n1: 1835
n2: 915 |
Arm1: 3
Arm2: |
Arm1:49.1
Arm2: 51.5 |
42 |
ITT |
Arm1: 1.3
Arm2: 2.6 |
Arm1:BNT162b2(3µg)
Arm2: Placebo |
Arm1:9
Arm2: 13 |
71.8 (28.6, 89.4) |
| Sadoff (2022) 43 |
USA |
Healthy adults |
total: 43788
n1: 21898
n2: 21890 |
Arm1: 52
Arm2: 52 |
Arm1:55.1
Arm2: |
120 |
PP |
Arm1: 10.6
Arm2: 10.4 |
Arm1:Ad26.COV2.S
Arm2: Placebo |
Arm1:433
Arm2: 883 |
52.9 (47.1, 58.1) |
| Sobieszczyk (2022) 44 |
USA |
Healthy adults |
total: 32450
n1: 21634
n2: 10816 |
Arm1: 51
Arm2: 51 |
Arm1:55.5
Arm2: 55.5 |
78 |
interim analysis |
Arm1: 9.5
Arm2: 18.0 |
Arm1:AZD1222
Arm2: Placebo |
Arm1:335
Arm2: 224 |
67.0 (58.9, 73.4) |
| S. J. Thomas (2021) 45 |
USA |
Healthy adults |
total: 44165
n1: 22085
n2: 22080 |
Arm1: 51
Arm2: 51 |
Arm1:51.3
Arm2: 50.0 |
180 |
PP |
Arm1: 1.5
Arm2: |
Arm1:BNT162b2(30µg)
Arm2: Placebo |
Arm1:3
Arm2: 35 |
91.3 (89.0, 93.2) |
| Toback (2021) 46 |
UK |
Healthy adults |
total: 15187
n1: 217
n2: 214
n3:502
n4:497 |
Arm1: 42.3
Arm2: 41.9
Arm2: 51.6
Arm2: 51.4 |
Arm1:56.7
Arm2: 55.1
Arm2: 51.4
Arm2: 58.4 |
60 |
ITT |
Arm1: 0.0
Arm2: 0.0
Arm3: 0.0
Arm3: 0.0 |
Arm1:NVX-CoV2373(5µg) + influenza
Arm2: Placebo + influenza
Arm2: NVX-CoV2373(5µg)
Arm2: Placebo |
Arm1:2
Arm2: 8
Arm3: 1
Arm4: 8 |
87.5 (0.2, 98.4) |
| Torales (2022) 47 |
Paraguay |
Healthy adults |
total: 1105
n1: 520
n2: 510 |
Arm1: 32.1
Arm2: 32.2 |
Arm1:58.5
Arm2: 61.8 |
28 |
interim analysis |
Arm1: 10.4
Arm2: 10.0 |
Arm1:MVC-COV1901
Arm2: AZD1222 |
Arm1: NR
Arm2: NR |
62.6 (50.9, 71.5) |
| Walter (2022) 48 |
USA |
Children |
total: 2285
n1: 1528
n2: 757 |
Arm1: 8.2
Arm2: 8.1 |
Arm1:52.3
Arm2: 50.6 |
69 |
ITT |
Arm1: 1.2
Arm2: 1.5 |
Arm1:BNT162b2(30µg)
Arm2: Placebo |
Arm1:3
Arm2: 16 |
90.7 (67.4, 98.3) |
| Winokur (2022) 49 |
USA |
Healthy adults |
total: 1846
n1: 306
n2: 302
n3: 308
n4: 308
n5: 306
n6: 316 |
Arm1: 66
Arm2: 67
Arm2: 67
Arm2: 67
Arm2: 67
Arm2: 67 |
Arm1:47.4
Arm2: 48.0
Arm2: 50.0
Arm2: 49.7
Arm2: 52.9
Arm2: 48.4 |
51 |
ITT |
Arm1: 1.3
Arm2: 0.3
Arm3: 1.0
Arm4: 1.3
Arm5: 0.7
Arm6: 0.9 |
Arm1:BNT162b2(30µg)
Arm2: BNT162b2(60µg)
Arm3: monovalent BA.1(30µg)
Arm4: monovalent BA.1(60µg)
Arm5: bivalent BA.1(30µg)
Arm6: bivalent BA.1(60µg) |
Arm1:7
Arm2: 6
Arm3: 7
Arm4: 3
Arm5: 1
Arm6: 6 |
NR |
| Mohraz (2023) 50 |
Iran |
Healthy adults |
total: 20000
n1: 13335
n2: 6665 |
Arm1: 38.3
Arm2: 38.2 |
Arm1: 65.5
Arm2: 65.4 |
83 |
PP |
Arm1: 0.49
Arm2: 0.23 |
Arm1: BIV1-CovIran
Arm2: Placebo |
Arm1: 758
Arm2: 688 |
50.2 (44.7, 55.0) |
Note. PP: Per-protocol; ITT: Intention to treat; NR: Not reported; CI: Confidence interval.
The incidence of confirmed cases of symptomatic COVID-19 among adults has been reported in 25 RCTs. These RCTs formed two subnetworks involving 23 vaccines and 20 designs. The first subnetwork entails 24 RCTs with 24 pairwise comparisons, 20 vaccines, one placebo, and 19 designs. Figure 3 illustrates the visual presentation of this network. The I2 value for this network was 84.7%, and the p-value for heterogeneity testing (within the design) was < 0.001. There was no indication of publication bias in this NMA, as the P value of the Egger test was 0.308.
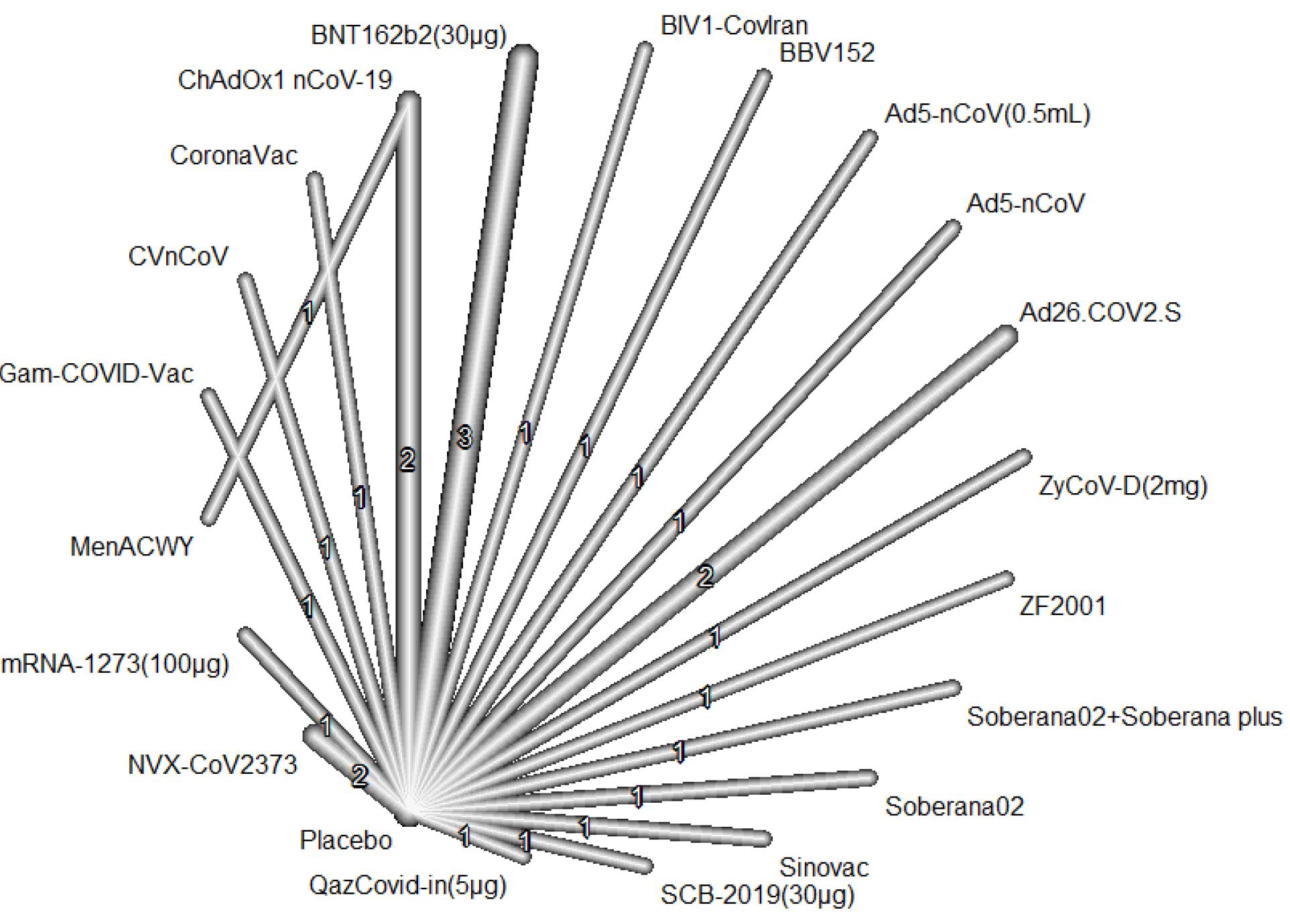
Figure 3.
The network plot of the available COVID-19 vaccines compared in phase three trials
.
The network plot of the available COVID-19 vaccines compared in phase three trials
The efficacy of vaccines has been reported in 27 RCTs. The highest reported efficacy (99.0%; 95% CI: 75.0, 100.0) was associated with BNT162b2 (30 µg), according to Table 1.
Based on the results of the NMA and the simultaneous comparison of all vaccines versus placebo, mRNA-1273 was the most effective vaccine in preventing COVID-19, and the highest P-score (0.93) was associated with this vaccine. The RR for mRNA-1273 versus placebo was 0.07 (95% CI: 0.03, 0.17). The second- and third-ranked vaccines were BNT-162b2 (RR = 0.08; 95% CI: 0.04, 0.15; P-score = 0.93) and Gam-COVID-Vac (RR = 0.09; 95% CI: 0.03, 0.25; P-score = 0.88). Overall, all vaccines, except for MenACWY, were significantly effective in preventing COVID-19 (Figure 4). The pooled comparisons of all vaccines are presented in Table S2 (see Supplementary file 1). The vaccines in a three-arm RCT were not connected to the network.24 In this study, two inactivated vaccines, including SARS-CoV-2 WIV04 and HB02, were compared with aluminum hydroxide. Based on the results of this study, the vaccine efficacy for WIV04 and HB02 was 72.8% and 78.1%, respectively.
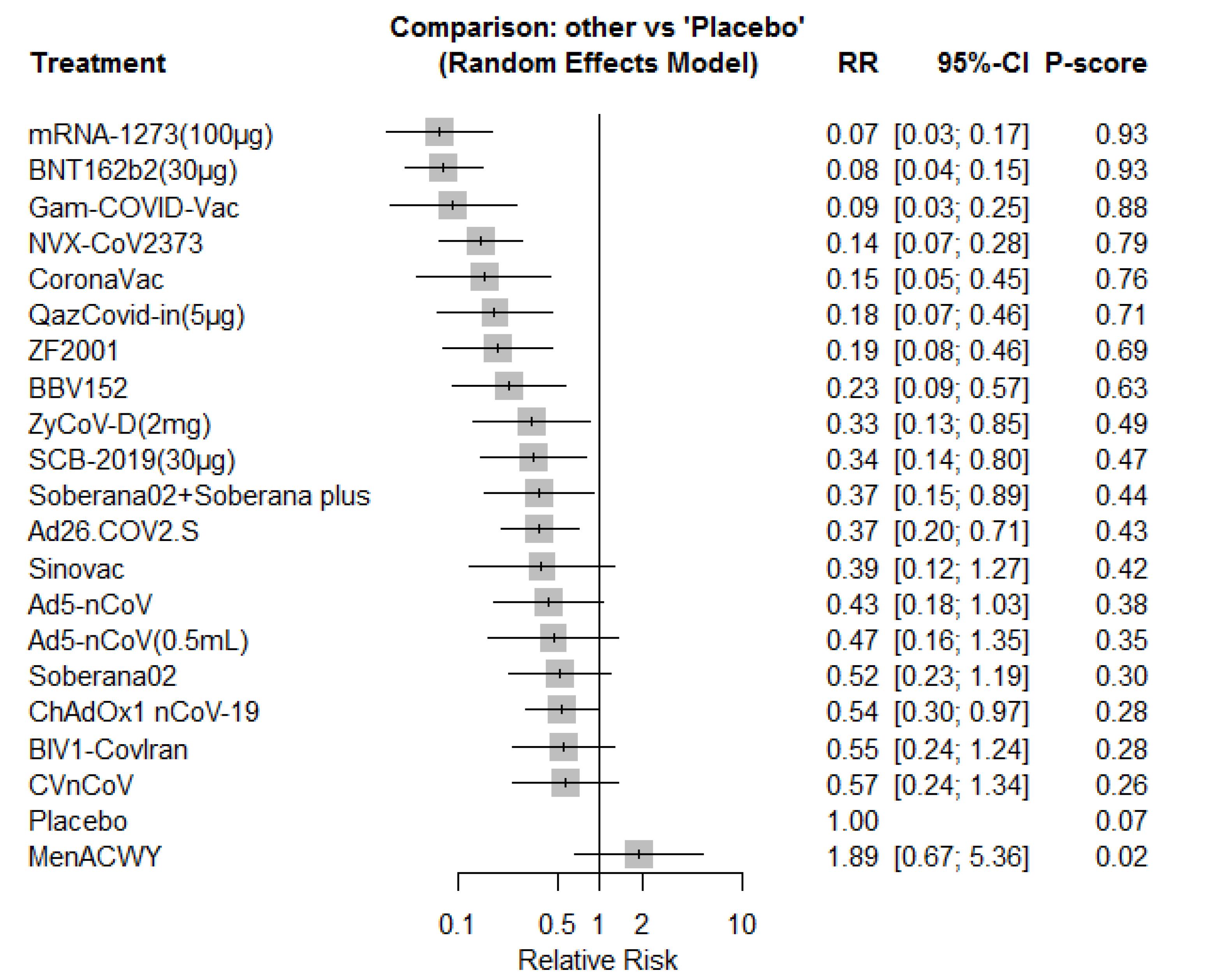
Figure 4.
The forest plot for the comparison of the available COVID-19 vaccines versus placebo in the network meta-analysis
.
The forest plot for the comparison of the available COVID-19 vaccines versus placebo in the network meta-analysis
The included RCTs evaluating the vaccines in children were five RCTs24,26,32,42,48 with six pairwise comparisons, five interventions, and four designs. The visual representation of the vaccine network is depicted in Figure S1(see Supplementary file 1). The I2 value for this network and the P value for the test of heterogeneity (within design) were 0 and 0.710, respectively. In children, the highest efficacy was associated with BNT162b2 (30 µg, 99.0%; 95% CI: 75.3, 100.0) in an RCT by Frenck et al32 (Table 1).
Based on the results of the NMA, BNT162b2 (30 µg) was the most effective vaccine in children (P-score = 0.84). The RR for comparing BNT162b2 (30 µg) with a placebo was 0.08 (95% CI: 0.03, 0.24). Overall, all vaccines were effective in preventing COVID-19 in this group compared to placebo Figure S2 (see Supplementary file 1). The pooled comparisons of all vaccines in this group are provided in Table S3 (see Supplementary file 1).
Two RCTs were conducted on people over 55 years of age. In the study by Sadoff et al comparing single-dose Ad26.CoV2.S with a placebo, vaccine efficacy ≥ 14 days and ≥ 28 days after administration was 55.0% (95% CI: 42.9, 64.7) and 46.6% (95% CI: 30.7, 59.0), respectively.43 In another RCT by Winokur et al, BNT162b2 (30 µg), BNT162b2 (60 µg), monovalent BA.1 (30 µg), monovalent BA.1 (60 µg), bivalent BA.1 (30 µg), and bivalent BA.1 (60 µg) were compared, there was no significant difference among the mentioned vaccines in terms of the incidence of confirmed cases of COVID-19 after administration.49
Table 2 summarizes the RR for the incidence of major vaccine complications, including local reactions, fatigue, chills, fever, pain, and headache. Based on the results of NMA for the mentioned complications, the risk of local reaction for Ad5-nCoV (0.5 mL) was the highest compared with a placebo among RCTs reporting this complication. The risks of fatigue, chills, fever, pain, and headache were the highest for Sinovac, BNT162b2, BNT162b2, Sinovac, and BNT162b2 (30 µg), respectively. Among children, BNT162b2 was associated with the highest risk of the above-mentioned complications. The simultaneous comparisons of the vaccines for the incidence of local reactions, fatigue, chills, fever, pain, and headache are listed in Tables S4-S9(see Supplementary file 1).
Table 2.
The relative risk for the complications of each vaccine versus the placebo
|
Vaccines
|
Local Reaction
|
Fatigue
|
Chill
|
Fever
|
Pain
|
Headache
|
| Ad26.CoV2.S |
3.04 (2.51, 3.67) |
1.89 (1.48, 2.42) |
Unreported |
Unreported |
2.69 (2.08, 3.47) |
1.84 (1.49, 2.27) |
| Ad5-nCoV |
3.09 (2.33, 4.10) |
1.68 (0.56, 5.09) |
Unreported |
7.92 (1.46, 42.83) |
2.13 (1.47, 3.07) |
1.45 (1.07, 1.97) |
| Ad5-nCoV (0·5 mL) |
17.86 (4.37, 72.92) |
Unreported |
Unreported |
3.16 (0.53, 18.73) |
0.34 (0.17, 0.69) |
1.24 (0.49, 3.11) |
| BIV1-CovIran |
1.08 (0.83, 1.39) |
3.37 (2.73, 4.15) |
Unreported |
Unreported |
Unreported |
Unreported |
| BNT162b2 (30 µg) |
7.36 (6.24, 8.68) |
1.67 (1.19, 2.35) |
11.05 (7.31, 16.71) |
Unreported |
5.34 (4.24, 6.74) |
2.88 (2.40, 3.46) |
| ChAdOx1 nCoV-19 |
2.5 (1.74, 3.59) |
1.19 (0.83, 1.70) |
3.96 (2.10, 7.48) |
Unreported |
3.59 (2.50, 5.17) |
1.77 (1.33, 2.36) |
| CoronaVac |
1.75 (1.20, 2.56) |
2.71 (1.91, 3.84) |
1.28 (0.64, 2.54) |
1.22 (0.23, 6.47) |
1.32 (0.89, 1.97) |
0.96 (0.70, 1.32) |
| CVnCoV |
5.54 (4.18, 7.35) |
Unreported |
9.89 (5.02, 19.46) |
92.34 (14.40, 592.22) |
5.91 (4.04, 8.65) |
3.07 (2.27, 4.15) |
| Gam-COVID-Vac |
0.55(0.33,0.90) |
Unreported |
Unreported |
1.33 (0.09, 20.45) |
0.83 (0.16, 4.43) |
1.11 (0.50, 2.45) |
| mRNA-1273 (100 µg) |
4.72 (3.66, 6.09) |
2.81 (2.01, 3.93) |
7.99 (4.22, 15.13) |
52.92 (10.03, 279.34) |
4.68 (3.31, 6.61) |
2.52 (1.90, 3.34) |
| MVC-CoV1901 |
2.6 (1.59, 4.26) |
1.93 (1.05, 3.55) |
5.44 (1.79, 16.49) |
Unreported |
4.7 (2.48, 8.89) |
1.77 (1.05, 2.99) |
| NVX-CoV2373 |
3.76 (2.91, 4.86) |
2.34 (1.67, 3.28) |
Unreported |
21.16 (3.91, 114.36) |
4.12 (2.91, 5.84) |
2.34 (1.76, 3.12) |
| Placebo |
1.00 |
1.00 |
1.00 |
1.00 |
1.00 |
1.00 |
| QazCOVID-in (5 µg) |
3.75 (2.25, 6.25) |
0.25 (0.03, 1.82) |
0.38 (0.09, 1.54) |
0.47 (0.07, 2.97) |
0.31 (0.08, 1.21) |
0.75 (0.39, 1.45) |
| SCB-2019 (30 µg) |
3.47 (2.36, 5.11) |
1.35 (0.86, 2.12) |
1.92 (0.75, 4.92) |
2.50 (0.25, 25.33) |
1.20 (0.71, 2.04) |
1.10 (0.74, 1.64) |
| Sinovac |
3.48 (2.19, 5.52) |
6.27 (2.66, 14.81) |
Unreported |
2.00 (0.19, 21.04) |
8.98 (4.03, 20.00) |
Unreported |
| Soberana02 |
2.49 (1.92, 3.24) |
1.2 (0.85, 1.70) |
1.05 (0.52, 2.13) |
1.16 (0.22, 5.99) |
1.29 (0.87, 1.91) |
1.07 (0.79, 1.44) |
| Soberana02 + Soberana plus |
2.66 (1.93, 3.66) |
1.21 (0.79, 1.85) |
1.25 (0.36, 4.34) |
1.64 (0.30, 8.92) |
2.39 (1.18, 4.84) |
1.11 (0.74, 1.67) |
| ZyCoV-D (2s mg) |
1.06 (0.62, 1.82) |
0.65 (0.28, 1.48) |
Unreported |
1.23 (0.21, 7.39) |
1.17 (0.50, 2.71) |
0.95 (0.49, 1.85) |
Discussion
In this NMA, the available vaccines (20 vaccines versus a placebo) were ranked for the prevention of symptomatic COVID-19. Based on the results of this study, mRNA-1273, BNT162b2, and Gam-COVID-Vac were the most effective vaccines in adults. In children, BNT162b2 was the most effective vaccine. Overall, all vaccines, except for MenACWY, were significantly effective in preventing COVID-19 in adults. Local reactions, fatigue, chills, fever, pain, and headaches were the common complications in the included RCTs. The risk of these complications was the highest for Ad5-nCoV (0.5 mL), Sinovac, BNT162b2 (30 µg), BNT162b2 (30 µg), Sinovac, and BNT162b2 (30 µg) versus a placebo, respectively. In this NMA, the previously published NMAs were updated, and the latest published RCTs were included in this study.
In a published NMA of nine vaccines, BNT162b2 mRNA-1273, followed by Gam-COVID-Vac, were ranked with the highest probability of efficacy against symptomatic COVID-19.11 Our results are in line with a published NMA in 2022, showing that BNT162b2, mRNA-1273, and rAd26&rAd5 (Gam-COVID-Vac) were the three best vaccines, respectively.12 The results of a previously published NMA from 2021 aligned with our findings concerning symptomatic COVID-19 prevention.13 According to this NMA, Pfizer, Moderna, and Sputnik were the most effective vaccines, which is consistent with our results. Our study added value to the previous NMA by simultaneously comparing 20 vaccines. Overall, our findings confirmed those of prior NMA studies.
In this study, comparing different doses of BNT162b2 and mRNA-1273 mRNA vaccines in children and adolescents, all doses were effective in preventing symptomatic COVID-19. However, BNT162b2 (30 μg) was found to be the most effective vaccine. These findings align with other published NMAs, suggesting that mRNA vaccines are the most effective in preventing symptomatic COVID-19. Despite opposition from some companies regarding the use of mRNA-based vaccines,51 it appears that these platforms are effective in fighting the pandemic. Unlike protein-based vaccines that primarily stimulate antibody production, mRNA vaccines elicit both cellular and hormonal immune responses.52
In addition to vaccine efficacy and disease prevention, the safety and incidence of complications are crucial considerations in vaccine use. The included RCTs reported varying complication profiles. To address this issue, our NMA analyzed the risk of commonly reported complications such as local reactions, fatigue, chills, fever, pain, and headaches. Based on our findings, the highest risk for local reactions, fatigue, chills, fever, pain, and headaches occurred for Ad5-nCoV (0.5 mL), as well as for the Sinovac and BNT162b2 vaccines. According to an NMA, Pfizer, QazCOVID-in, and Clover vaccines have the highest risk for local side effects. In terms of systemic side effects, the ZyCoV-D, V591, V-01, and Sinopharm vaccines were the safest options, while the Pfizer, Clover, and QazCOVID-in vaccines carried the highest risk of developing such effects.13 Vaccines, similar to any other medical intervention, come with potential complications. While common complications are identified in phases two and three of trials, the identification of rare complications requires phase four studies in post-licensing evaluations. Overall, the decision to introduce a new vaccine depends on the burden of the disease, vaccine efficacy and effectiveness, vaccine safety, and the costs and cost-effectiveness of the vaccine.16
The key advantage of this study over previous NMAs is its comparison of multiple vaccines. For instance, the NMA includes findings from RCTs conducted in Iran on Soberana 02, Soberana Plus,10 and BIV1-CovIran vaccines.50
We were unable to assess the consistency assumption in this NMA due to the absence of a closed loop in the vaccine network and the use of solely indirect estimates in the comparison of vaccines. Therefore, we could only evaluate the transitivity assumption qualitatively. Based on our evaluation of the transitivity assumption, we decided to conduct a subgroup NMA, including participants in different age groups [children and adolescents ( < 18 years old), adults (18-55 years old), and older adults ( > 55 years old)]. In this NMA, the available vaccines were ranked based on their ability to prevent symptomatic COVID-19. However, it is important to note that several factors, such as the virus strain, mutations, variations in the study population and setting, and the quality of the studies, were not accounted for in this NMA. Therefore, the results should be interpreted with caution.
Highlights
-
The twenty-three available COVID-19 vaccines were compared and ranked simultaneously.
-
All available vaccines are effective in preventing symptomatic COVID-19.
-
MRNA-1273 (Moderna) was the most effective vaccine for preventing COVID-19.
Conclusion
Based on the NMA results, all available vaccines have proven effective in preventing COVID-19. However, the top three ranked vaccines were mRNA-1273, BNT-162b2, and Gam-COVID-Vac, with the mRNA vaccines taking the lead. It is important to note that BNT-162b2 has a high risk of complications, including fatigue, chills, fever, pain, and headaches.
Acknowledgements
This study was part of the MSc thesis in epidemiology. We would like to thank the Health Sciences Research Center and the Vice-chancellor for Research and Technology of the Hamadan University of Medical Sciences for supporting this study.
Authors’ Contribution
Conceptualization: Amin Doosti-Irani.
Data curation: Shima Hossaini, Bushra Zareie, Amin Doosti-Irani.
Formal analysis: Amin Doosti-Irani and Shima Hossaini.
Investigation: Shima Hossaini, Fariba Keramat, Amin Doosti-Irani, Zahra Cheraghi.
Methodology: Amin Doosti-Irani, Shima Hossaini, Zahra Cheraghi.
Project administration: Amin Doosti-Irani.
Software: Amin Doosti-Irani, Shima Hossaini.
Supervision: Amin Doosti-Irani, Fariba Keramat.
Validation: Fariba Keramat, Zahra Cheraghi, Bushra Zarei, Amin Doosti-Irani.
Visualization: Amin Doosti-Irani, Shima Hossaini, Bushra Zareie.
Writing–original draft: Amin Doosti-Irani and Shima Hossaini.
Writing–review & editing: Amin Doosti-Irani, Zahra Cheraghi, Fariba Keramat, Shima Hossaini, Bushra Zareie.
Competing Interests
None.
Funding
None.
Supplementary Files
Supplementary file 1 contains Figure S1 and Tables S1-S9.
(pdf)
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int/?mapFilter=vaccinations. Updated July 10, 2023. Accessed July 24, 2023.
- Han X, Xu P, Ye Q. Analysis of COVID-19 vaccines: types, thoughts, and application. J Clin Lab Anal 2021; 35(9):e23937. doi: 10.1002/jcla.23937 [Crossref] [ Google Scholar]
- Korang SK, von Rohden E, Veroniki AA, Ong G, Ngalamika O, Siddiqui F. Vaccines to prevent COVID-19: a living systematic review with trial sequential analysis and network meta-analysis of randomized clinical trials. PLoS One 2022; 17(1):e0260733. doi: 10.1371/journal.pone.0260733 [Crossref] [ Google Scholar]
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N Engl J Med 2020; 383(27):2603-15. doi: 10.1056/NEJMoa2034577 [Crossref] [ Google Scholar]
- Tanriover MD, Doğanay HL, Akova M, Güner HR, Azap A, Akhan S. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet 2021; 398(10296):213-22. doi: 10.1016/s0140-6736(21)01429-x [Crossref] [ Google Scholar]
- Emary KRW, Golubchik T, Aley PK, Ariani CV, Angus B, Bibi S. Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B117): an exploratory analysis of a randomised controlled trial. Lancet 2021; 397(10282):1351-62. doi: 10.1016/s0140-6736(21)00628-0 [Crossref] [ Google Scholar]
- Logunov DY, Dolzhikova IV, Shcheblyakov DV, Tukhvatulin AI, Zubkova OV, Dzharullaeva AS. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021; 397(10275):671-81. doi: 10.1016/s0140-6736(21)00234-8 [Crossref] [ Google Scholar]
- Sadoff J, Gray G, Vandebosch A, Cárdenas V, Shukarev G, Grinsztejn B. Safety and efficacy of single-dose Ad26COV2S vaccine against COVID-19. N Engl J Med 2021; 384(23):2187-201. doi: 10.1056/NEJMoa2101544 [Crossref] [ Google Scholar]
- Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021; 384(5):403-16. doi: 10.1056/NEJMoa2035389 [Crossref] [ Google Scholar]
- Mostafavi E, Eybpoosh S, Karamouzian M, Khalili M, Haji-Maghsoudi S, Salehi-Vaziri M. Efficacy and safety of a protein-based SARS-CoV-2 vaccine: a randomized clinical trial. JAMA Netw Open 2023; 6(5):e2310302. doi: 10.1001/jamanetworkopen.2023.10302 [Crossref] [ Google Scholar]
- Rotshild V, Hirsh-Raccah B, Miskin I, Muszkat M, Matok I. Comparing the clinical efficacy of COVID-19 vaccines: a systematic review and network meta-analysis. Sci Rep 2021; 11(1):22777. doi: 10.1038/s41598-021-02321-z [Crossref] [ Google Scholar]
- Kumar S, Saikia D, Bankar M, Saurabh MK, Singh H, Varikasuvu SR. Efficacy of COVID-19 vaccines: a systematic review and network meta-analysis of phase 3 randomized controlled trials. Pharmacol Rep 2022; 74(6):1228-37. doi: 10.1007/s43440-022-00429-1 [Crossref] [ Google Scholar]
- Toubasi AA, Al-Sayegh TN, Obaid YY, Al-Harasis SM, AlRyalat SAS. Efficacy and safety of COVID-19 vaccines: a network meta-analysis. J Evid Based Med 2022; 15(3):245-62. doi: 10.1111/jebm.12492 [Crossref] [ Google Scholar]
- Oh S, Purja S, Shin H, et al. Efficacy, Immunogenicity, and Safety of COVID-19 Vaccines in Randomized Control Trials in the Pre-Delta Era: A Systematic Review and Network Meta-Analysis. Vaccines (Basel) 2022;10(10):1572. Published 2022 Sep 20. 10.3390/vaccines10101572.
- Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 2015; 162(11):777-84. doi: 10.7326/m14-2385 [Crossref] [ Google Scholar]
- Pebody R, Kretzschmar M. Principles and practice of vaccinology. In: Krämer A, Kretzschmar M, Krickeberg K, eds. Modern Infectious Disease Epidemiology: Concepts, Methods, Mathematical Models, and Public Health. New York, NY: Springer; 2010. p. 235-48. 10.1007/978-0-387-93835-6_14.
- Minozzi S, Cinquini M, Gianola S, Gonzalez-Lorenzo M, Banzi R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J Clin Epidemiol 2020; 126:37-44. doi: 10.1016/j.jclinepi.2020.06.015 [Crossref] [ Google Scholar]
- Review Manager (RevMan) [Computer program]. Version 5.4. The Cochrane Collaboration, 2020.
- Balduzzi S, Rücker G, Nikolakopoulou A, Papakonstantinou T, Salanti G, Efthimiou O. netmeta: an R package for network meta-analysis using frequentist methods. J Stat Softw 2023; 106(2):1-40. doi: 10.18637/jss.v106.i02 [Crossref] [ Google Scholar]
- Doosti-Irani A, Nazemipour M, Mansournia MA. What are network meta-analyses (NMAs)? A primer with four tips for clinicians who read NMAs and who perform them (methods matter series). Br J Sports Med 2021; 55(10):520-1. doi: 10.1136/bjsports-2020-102872 [Crossref] [ Google Scholar]
- Rücker G, Schwarzer G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol 2015; 15:58. doi: 10.1186/s12874-015-0060-8 [Crossref] [ Google Scholar]
- Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS One 2013; 8(10):e76654. doi: 10.1371/journal.pone.0076654 [Crossref] [ Google Scholar]
- Al Kaabi N, Zhang Y, Xia S, Yang Y, Al Qahtani MM, Abdulrazzaq N. Effect of 2 inactivated SARS-CoV-2 vaccines on symptomatic COVID-19 infection in adults: a randomized clinical trial. JAMA 2021; 326(1):35-45. doi: 10.1001/jama.2021.8565 [Crossref] [ Google Scholar]
- Ali K, Berman G, Zhou H, Deng W, Faughnan V, Coronado-Voges M. Evaluation of mRNA-1273 SARS-CoV-2 vaccine in adolescents. N Engl J Med 2021; 385(24):2241-51. doi: 10.1056/NEJMoa2109522 [Crossref] [ Google Scholar]
- Bravo L, Smolenov I, Han HH, Li P, Hosain R, Rockhold F. Efficacy of the adjuvanted subunit protein COVID-19 vaccine, SCB-2019: a phase 2 and 3 multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2022; 399(10323):461-72. doi: 10.1016/s0140-6736(22)00055-1 [Crossref] [ Google Scholar]
- Creech CB, Anderson E, Berthaud V, Yildirim I, Atz AM, Melendez Baez I. Evaluation of mRNA-1273 COVID-19 vaccine in children 6 to 11 years of age. N Engl J Med 2022; 386(21):2011-23. doi: 10.1056/NEJMoa2203315 [Crossref] [ Google Scholar]
- Dai L, Gao L, Tao L, Hadinegoro SR, Erkin M, Ying Z. Efficacy and safety of the RBD-dimer-based COVID-19 vaccine ZF2001 in adults. N Engl J Med 2022; 386(22):2097-111. doi: 10.1056/NEJMoa2202261 [Crossref] [ Google Scholar]
- Dunkle LM, Kotloff KL, Gay CL, Áñez G, Adelglass JM, Barrat Hernández AQ. Efficacy and safety of NVX-CoV2373 in adults in the United States and Mexico. N Engl J Med 2022; 386(6):531-43. doi: 10.1056/NEJMoa2116185 [Crossref] [ Google Scholar]
- Ella R, Reddy S, Blackwelder W, Potdar V, Yadav P, Sarangi V. Efficacy, safety, and lot-to-lot immunogenicity of an inactivated SARS-CoV-2 vaccine (BBV152): interim results of a randomised, double-blind, controlled, phase 3 trial. Lancet 2021; 398(10317):2173-84. doi: 10.1016/s0140-6736(21)02000-6 [Crossref] [ Google Scholar]
- Fadlyana E, Rusmil K, Tarigan R, Rahmadi AR, Prodjosoewojo S, Sofiatin Y. A phase III, observer-blind, randomized, placebo-controlled study of the efficacy, safety, and immunogenicity of SARS-CoV-2 inactivated vaccine in healthy adults aged 18-59 years: an interim analysis in Indonesia. Vaccine 2021; 39(44):6520-8. doi: 10.1016/j.vaccine.2021.09.052 [Crossref] [ Google Scholar]
- Falsey AR, Sobieszczyk ME, Hirsch I, Sproule S, Robb ML, Corey L. Phase 3 safety and efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 vaccine. N Engl J Med 2021; 385(25):2348-60. doi: 10.1056/NEJMoa2105290 [Crossref] [ Google Scholar]
- Frenck RW Jr, Klein NP, Kitchin N, Gurtman A, Absalon J, Lockhart S. Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. N Engl J Med 2021; 385(3):239-50. doi: 10.1056/NEJMoa2107456 [Crossref] [ Google Scholar]
- Gilbert PB, Montefiori DC, McDermott AB, Fong Y, Benkeser D, Deng W. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022; 375(6576):43-50. doi: 10.1126/science.abm3425 [Crossref] [ Google Scholar]
- Halperin SA, Ye L, MacKinnon-Cameron D, Smith B, Cahn PE, Ruiz-Palacios GM. Final efficacy analysis, interim safety analysis, and immunogenicity of a single dose of recombinant novel coronavirus vaccine (adenovirus type 5 vector) in adults 18 years and older: an international, multicentre, randomised, double-blinded, placebo-controlled phase 3 trial. Lancet 2022; 399(10321):237-48. doi: 10.1016/s0140-6736(21)02753-7 [Crossref] [ Google Scholar]
- Hardt K, Vandebosch A, Sadoff J, Le Gars M, Truyers C, Lowson D. Efficacy, safety, and immunogenicity of a booster regimen of Ad26COV2S vaccine against COVID-19 (ENSEMBLE2): results of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Infect Dis 2022; 22(12):1703-15. doi: 10.1016/s1473-3099(22)00506-0 [Crossref] [ Google Scholar]
- Heath PT, Galiza EP, Baxter DN, Boffito M, Browne D, Burns F. Safety and efficacy of the NVX-CoV2373 coronavirus disease 2019 vaccine at completion of the placebo-controlled phase of a randomized controlled trial. Clin Infect Dis 2023; 76(3):398-407. doi: 10.1093/cid/ciac803 [Crossref] [ Google Scholar]
- Khairullin B, Zakarya K, Orynbayev M, Abduraimov Y, Kassenov M, Sarsenbayeva G. Efficacy and safety of an inactivated whole-virion vaccine against COVID-19, QazCovid-in®, in healthy adults: a multicentre, randomised, single-blind, placebo-controlled phase 3 clinical trial with a 6-month follow-up. EClinicalMedicine 2022; 50:101526. doi: 10.1016/j.eclinm.2022.101526 [Crossref] [ Google Scholar]
- Khobragade A, Bhate S, Ramaiah V, Deshpande S, Giri K, Phophle H. Efficacy, safety, and immunogenicity of the DNA SARS-CoV-2 vaccine (ZyCoV-D): the interim efficacy results of a phase 3, randomised, double-blind, placebo-controlled study in India. Lancet 2022; 399(10332):1313-21. doi: 10.1016/s0140-6736(22)00151-9 [Crossref] [ Google Scholar]
- Kremsner PG, Ahuad Guerrero RA, Arana-Arri E, Aroca Martinez GJ, Bonten M, Chandler R. Efficacy and safety of the CVnCoV SARS-CoV-2 mRNA vaccine candidate in ten countries in Europe and Latin America (HERALD): a randomised, observer-blinded, placebo-controlled, phase 2b/3 trial. Lancet Infect Dis 2022; 22(3):329-40. doi: 10.1016/s1473-3099(21)00677-0 [Crossref] [ Google Scholar]
- Lioznov D, Amosova I, Sheetikov SA, Zornikova KV, Serdyuk Y, Efimov GA. Immunogenicity and safety of a recombinant adenovirus type-5 COVID-19 vaccine in adults: data from a randomised, double-blind, placebo-controlled, single-dose, phase 3 trial in Russia. PLoS One 2023; 18(3):e0278878. doi: 10.1371/journal.pone.0278878 [Crossref] [ Google Scholar]
- Moreira ED Jr, Kitchin N, Xu X, Dychter SS, Lockhart S, Gurtman A. Safety and efficacy of a third dose of BNT162b2 COVID-19 vaccine. N Engl J Med 2022; 386(20):1910-21. doi: 10.1056/NEJMoa2200674 [Crossref] [ Google Scholar]
- Muñoz FM, Sher LD, Sabharwal C, Gurtman A, Xu X, Kitchin N. Evaluation of BNT162b2 COVID-19 vaccine in children younger than 5 years of age. N Engl J Med 2023; 388(7):621-34. doi: 10.1056/NEJMoa2211031 [Crossref] [ Google Scholar]
- Sadoff J, Gray G, Vandebosch A, Cárdenas V, Shukarev G, Grinsztejn B. Final analysis of efficacy and safety of single-dose Ad26COV2S. N Engl J Med 2022; 386(9):847-60. doi: 10.1056/NEJMoa2117608 [Crossref] [ Google Scholar]
- Sobieszczyk ME, Maaske J, Falsey AR, Sproule S, Robb ML, Frenck RW Jr. Durability of protection and immunogenicity of AZD1222 (ChAdOx1 nCoV-19) COVID-19 vaccine over 6 months. J Clin Invest 2022; 132(18):e160565. doi: 10.1172/jci160565 [Crossref] [ Google Scholar]
- Thomas SJ, Moreira ED Jr, Kitchin N, Absalon J, Gurtman A, Lockhart S. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine through 6 months. N Engl J Med 2021; 385(19):1761-73. doi: 10.1056/NEJMoa2110345 [Crossref] [ Google Scholar]
- Toback S, Galiza E, Cosgrove C, Galloway J, Goodman AL, Swift PA. Safety, immunogenicity, and efficacy of a COVID-19 vaccine (NVX-CoV2373) co-administered with seasonal influenza vaccines: an exploratory substudy of a randomised, observer-blinded, placebo-controlled, phase 3 trial. Lancet Respir Med 2022; 10(2):167-79. doi: 10.1016/s2213-2600(21)00409-4 [Crossref] [ Google Scholar]
- Torales J, Cuenca-Torres O, Barrios L, Armoa-Garcia L, Estigarribia G, Sanabria G. An evaluation of the safety and immunogenicity of MVC-COV1901: results of an interim analysis of a phase III, parallel group, randomized, double-blind, active-controlled immunobridging study in Paraguay. Vaccine 2023; 41(1):109-18. doi: 10.1016/j.vaccine.2022.10.030 [Crossref] [ Google Scholar]
- Walter EB, Talaat KR, Sabharwal C, Gurtman A, Lockhart S, Paulsen GC. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N Engl J Med 2022; 386(1):35-46. doi: 10.1056/NEJMoa2116298 [Crossref] [ Google Scholar]
- Winokur P, Gayed J, Fitz-Patrick D, Thomas SJ, Diya O, Lockhart S. Bivalent Omicron BA1-adapted BNT162b2 booster in adults older than 55 years. N Engl J Med 2023; 388(3):214-27. doi: 10.1056/NEJMoa2213082 [Crossref] [ Google Scholar]
- Mohraz M, Vahdat K, Ghamari SH, Abbasi-Kangevari M, Ghasemi E, Ghabdian Y. Efficacy and safety of an inactivated virus-particle vaccine for SARS-CoV-2, BIV1-CovIran: randomised, placebo controlled, double blind, multicentre, phase 3 clinical trial. BMJ 2023; 382:e070464. doi: 10.1136/bmj-2023-070464 [Crossref] [ Google Scholar]
- Mirtaleb MS, Falak R, Heshmatnia J, Bakhshandeh B, Taheri RA, Soleimanjahi H. An insight overview on COVID-19 mRNA vaccines: advantageous, pharmacology, mechanism of action, and prospective considerations. Int Immunopharmacol 2023; 117:109934. doi: 10.1016/j.intimp.2023.109934 [Crossref] [ Google Scholar]
- Schlake T, Thess A, Fotin-Mleczek M, Kallen KJ. Developing mRNA-vaccine technologies. RNA Biol 2012; 9(11):1319-30. doi: 10.4161/rna.22269 [Crossref] [ Google Scholar]