J Res Health Sci. 24(3):e00617.
doi: 10.34172/jrhs.2024.152
Review Article
Factors Influencing the Use of Tobacco Among Youth in Low-Income, Lower-Middle-Income, and Upper-Middle-Income Countries: A Systematic Review
Fahad Ali Mangrio 1  , Penpaktr Uthis 2, * , Suwimon Rojnawee 2
, Penpaktr Uthis 2, * , Suwimon Rojnawee 2
Author information:
1Nursing Student at the Faculty of Nursing, Chulalongkorn University, Bangkok, Thailand
2Faculty of Nursing, Chulalongkorn University, Bangkok, Thailand
Abstract
Background: The use of tobacco is a significant global public health issue. According to the World Health Organization, tobacco use is a considerable risk factor for many diseases and causes more than 8 million deaths per year, with a disproportionate impact on low- and middle-income countries. Therefore, this systematic review was conducted to identify the factors influencing tobacco use among youth in low-income, lower-middle-income, and upper-middle-income countries.
Study Design: A system review.
Methods: The review followed the PRISMA guidelines, and the protocol was registered on PROSPERO (CRD42023430552). Several data sources were utilized, including PubMed, Scopus, ScienceDirect, MEDLINE, CINAHL, and ProQuest, and cross-sectional data from participants aged 15‒24 underwent investigation. Original full-text articles have been published between 2015 and 2023. Out of the 2892 studies, 20 were included in this review after two reviewers confirmed the eligibility criteria.
Results: The average age of the participants was (mean±standard deviation: 19.45±1.686). Most studies were conducted in lower-middle and upper-middle-income countries. Frequently reported influences were at the individual and social levels, including demographic, economic, and psychological parameters, attitude and knowledge, individual behavioral factors, parental education, family member tobacco use, stressful life events, and social networks. At the environmental level, factors included secondhand smoke exposure, community context, media channels, and access to tobacco.
Conclusion: The findings demonstrated a significant association between youth tobacco use and individual-, social-, and environmental-level factors. Consequently, specific interventions targeting these factors should be deployed to mitigate youth tobacco use in various socioeconomic settings.
Keywords: Influential factors, Tobacco use, Youth, Low-income, Lower-middleincome, Upper-middle-income, Countries
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Mangrio FA, Uthis P, Rojnawee S. Factors influencing the use of tobacco among youth in low-income, lower-middle-income, and upper-middle-income countries: a systematic review. J Res Health Sci. 2024; 24(2):e00617. doi:10.34172/jrhs.2024.152
Background
The use of tobacco among youth presents a substantial public health concern worldwide, with significant implications for their physical, mental, and social well-being.1 Tobacco use has primarily been defined as the consumption of tobacco products such as pipes, cigarillos, water pipes, locally grown tobacco, and smokeless tobacco products.2 Evidence has shown that approximately 80% of the global tobacco consumer population, which amounts to around 1.3 billion individuals, resides in low- and middle-income countries.3 The World Health Organization reported that tobacco use is responsible for six million deaths worldwide, with an additional 600 000 deaths attributed to secondhand smoke exposure.4 The frequency of tobacco use among youth differs across countries, and the overall prevalence of tobacco use is 19.33% across 133 low-income and middle-income countries.5 Tobacco use significantly decreases in high-income countries compared to low- and middle-income countries. For instance, in Australia, the prevalence of youth tobacco consumption has reduced from 7.0% to 3.0%6; in contrast, the prevalence of tobacco use among youth in low- and middle-income countries, such as Madagascar (23.75%),5 Nepal (20.5%), and Haiti (19.75%), has demonstrated an increase.7 In addition, a systematic review found extensive variations in tobacco use proportion, ranging from 2% to over 30%, depending on the geographical location and specific tobacco products.8
Tobacco use is a significant risk factor for various chronic diseases, such as cancer, cardiovascular diseases, mental health issues, and respiratory diseases.6 The burden of morbidity and mortality from these diseases is strongly linked with tobacco use in low-income, lower-middle-income, and upper-middle-income countries.8 Moreover, tobacco consumption impacts the spread of poverty and inequality by diverting household resources away from essential needs, subsequently reducing productivity and income, and increasing healthcare expenditures.9 Further, tobacco use has harmful environmental impacts that adversely affect the livelihood and well-being of individuals in low- and middle-income countries.10
The World Bank ranks world economies into four group classes of income in July each year based on gross national income per capita.11,12 The present group classification identifies 26 countries as low-income and 108 as middle-income, further divided into 60 upper-middle-income and 48 lower-middle-income countries.11 Overall, these countries account for approximately 75% of the global population and contribute to 40% of the world’s economic activity.12 These outcomes emphasize the necessity of coordinated attempts to reduce tobacco consumption among youth in low-income, lower-middle-income, and middle-income countries.
The youth populations are specifically prone to engaging in tobacco use due to the influence of numerous factors such as peer pressure, social norms, and targeted marketing schemes used by the tobacco industry.13 The early initiation of tobacco use has profound effects on both physical and cognitive development.14 Individuals who initiate tobacco smoking at an early age are more prone to developing tobacco addiction and face greater challenges when struggling to quit smoking in adulthood.15 A further systematic review suggested that most studies were conducted in high-income countries, despite youth smoking rates being substantially higher in lower- and middle-income countries.16 Moreover, understanding the socioeconomic determinants of youth tobacco smoking is crucial for effective interventions.17 Therefore, it is necessary to conduct research on factors affecting tobacco use within diverse socioeconomic contexts to develop tailored interventions and address the consequences of tobacco-related diseases and disparities. Significantly, based on the current body of knowledge, this systematic review represents the first comprehensive examination of factors associated with tobacco use among youth in low-income, lower-middle-income, and upper-middle-income countries.
The primary objective of this systematic review was to investigate factors influencing tobacco use among youth in low-income, lower-middle-income, and upper-middle-income countries.
Methods
Study design
This systematic review followed the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).18 The review adhered to the 27-item checklist and revised the flowchart provided in the PRISMA guidelines. The protocol for this systematic review was registered in PROSPERO (CRD42023430552).
Population, exposure, comparison, outcome, and study design criteria
Population: It included individuals who fall within the age range of 15‒24, as defined by the United Nations youth definition,19,20 and who have used any form of tobacco (i.e., cigarettes, cigars, smokeless tobacco, hookah, heated tobacco products, nicotine pouches, or e-cigarettes) within the last 30 days. Additionally, these individuals reside in countries that fall under the classification of low-income, lower-middle-income, or upper-middle-income, as determined by the World Bank.12
Exposure: Influencing factors.
Comparison: No.
Outcomes: Tobacco use among youth.
Study design: Cross-sectional.
Selection criteria
The study was based on original research and available full texts. To ensure the inclusion of the most up-to-date findings and credible evidence for timely decisions, the publication period of studies for this systematic review was restricted from 2015 to 2023.21-23
Search strategy
Multiple databases, such as PubMed, Scopus, ScienceDirect, MEDLINE, CINAHL, and ProQuest, were extensively searched using generated MeSH (Medical Subject Headings) terms and keywords.They included factors influencing OR predictors influencing OR identifying factors OR associated factors AND tobacco abuse OR cigarette consumption OR chewing tobacco OR smokeless tobacco, AND youth OR young people OR adolescents. After searching, the studies were selected in accordance with the 2022 World Bank Index of Economic Classifications,12 which encompasses countries with low-income, lower-middle-income, and upper-middle-income status. Moreover, the investigators formulated and implemented search methodologies under the guidance of a skilled health science librarian.
Study selection
The initial search across databases yielded 2892 articles (Figure 1). Two independent reviewers screened the titles and abstracts of potential articles to determine the eligibility criteria. If an article potentially met the inclusion criteria, the complete article was obtained and reviewed to confirm eligibility and inclusion in the review. Disagreements between reviewers were resolved through discussion or the involvement of a third reviewer when necessary.
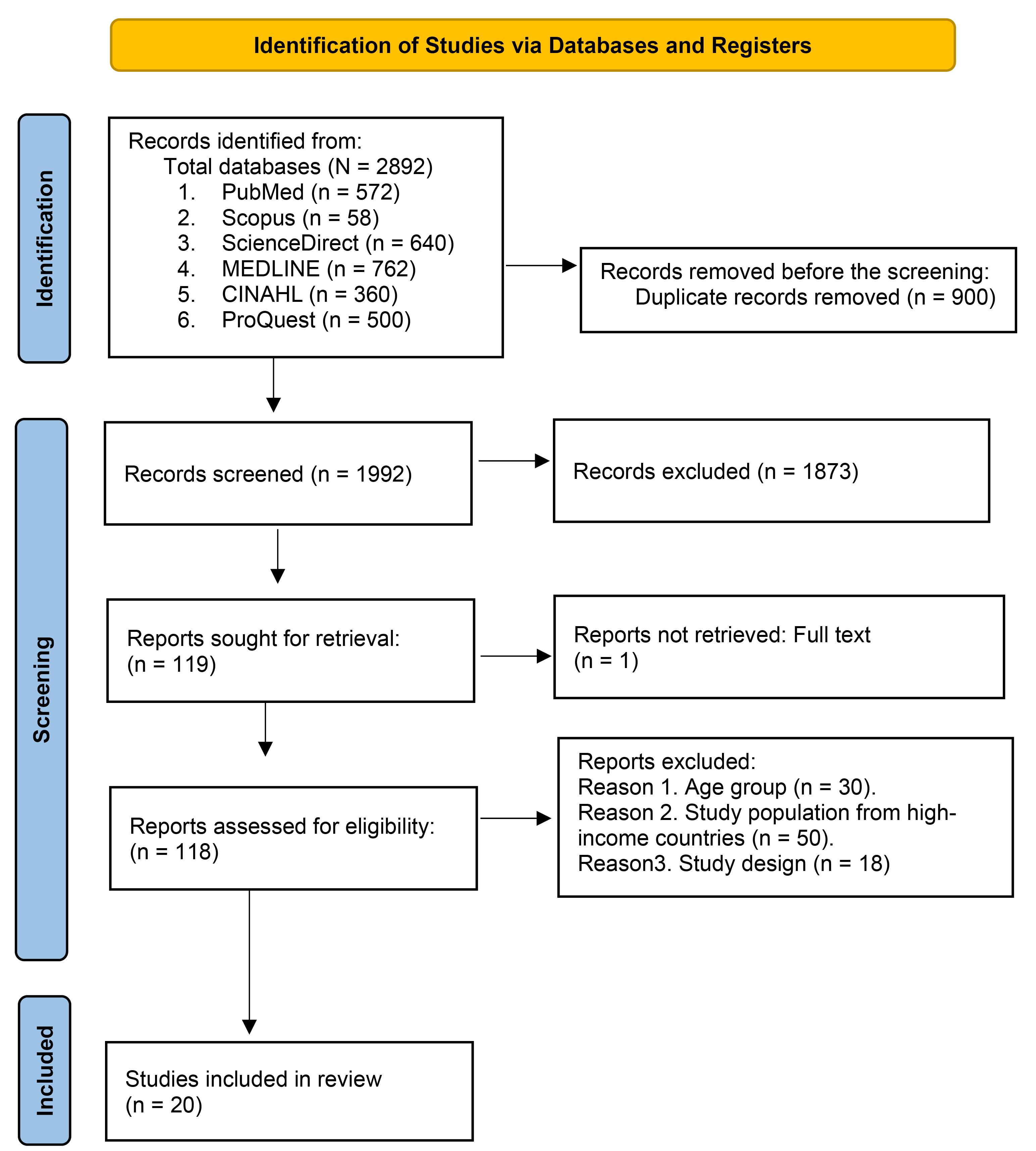
Figure 1.
PRISMA flow chart. Note. PRIMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
.
PRISMA flow chart. Note. PRIMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Nine hundred duplicate articles were removed using the EndNote 21 “find duplicate” library feature and manual inspection. During the title and abstract screening process, 1873 records were excluded based on failure to meet study eligibility criteria. Of these, 500 articles did not address factors associated with youth tobacco use, and the remaining 1373 articles were not specific to the study objective. In addition, one article did not retrieve the full text.24 Next, full-text versions were obtained for the remaining 118 articles. Two authors (F. A. M. and S. R.) independently reviewed these articles based on the inclusion and exclusion criteria. After the full-text review, 20 articles were determined to be eligible and included in this systematic review.
Data extraction
The data extracted from these studies were synthesized and summarized using the matrix method25 and the narrative synthesis technique.26 Table 1 presents a comprehensive summary of the included 20 studies, including author(s) name and year of publication, country economic status, age range, study design, sample size, measurement, prevalence of smoking and smokeless tobacco use, identified risk factors, statistical findings, and quality appraisal scores. Furthermore, all the text from the result summary was coded line-by-line for reported influences on tobacco use under individual-, social-, and environmental-level factors based on an adapted model of the Theory of Triadic Influence.27
Table 1.
Summary of the data from all eligible included studies
|
Author(s) name and year of publication
|
Country economic status
|
Age range
|
Study
design
|
Sample
size
|
Measurement
|
Prevalence of smoking and smokeless tobacco use
|
Identified risk factors
|
Statistical findings
OR (95% Cl)
|
Quality appraisal scores
|
|
Upper-middle-income countries
|
| Othman et al(2017) 28 |
Iraq |
18-24 |
Cross-sectional |
1,160 |
Self-report |
Cigarette (10.0%) and
waterpipe (28.0%) |
Male gender |
5.70 (3.90, 8.20) |
Strong |
| Drink alcohol and other substances |
2.80 (1.40, 5.60) |
| Chirtkiatsakul et al(2019) 29 |
Malaysia |
18-24 |
Cross-sectional |
843 |
Self-report |
Cigarette (22.4%) |
Male gender |
12.60 (8.04, 19.89) |
Moderate |
| Mothers with primary-level education |
4.02 (1.40, 11.50) |
| Favorable attitudes toward smoking |
9.09 (4.98, 16.50) |
| Equivocal attitudes |
2.98 (1.78, 5.00) |
| Suwanwong et al (2021)30 |
Thailand |
15-19 |
Cross-sectional |
6,046 |
Self-report |
Cigarette (6.4%) |
Male gender |
34.29 (16.60, 70.73) |
Strong |
| Alcohol use |
17.05 (12.87, 22.59) |
| Exposure secondhand smoke home |
6.63 (4.98, 8.82) |
| Exposure secondhand smoke school |
2.02 (1.38, 2.97) |
| Exposure secondhand smoke at restaurant |
1.57 (1.17, 2.10) |
| Public transport |
1.42 (1.02, 1.98) |
| Alcohol use |
17.05 (12.87, 22.59) |
| Tobacco advertising |
1.90 (1.31, 2.75) |
| Yusof et al (2019)31 |
Malaysia |
18-19 |
Cross-sectional |
388 |
Self-report |
E-cigarette (14.4%) |
Gender male |
25.70 (10.88, 60.71) |
Strong |
| Peer use of e-cigarettes |
19.93 (11.18, 35.55) |
| Todorović et al (2022)32 |
Bosnia & Herzegovina |
18-24 |
Cross-sectional |
1,200 |
Self-report |
Cigarette (34.1%) |
Secondhand smoke at home |
1.19 (1.09, 1.30) |
Strong |
| More money available |
1.19 (1.05, 1.34) |
| Gazibara et al (2021)33 |
Kosovo, Serbia |
17-21 |
Cross- section |
514 |
Self-report |
Cigarette (22.6%) |
Exposure secondhand smoke |
1.07 (1.01, 1.13) |
Strong |
| Severe depressive symptoms |
1.12 (1.07, 1.18) |
| Living with smokers |
3.78 (1.69, 8.07) |
| Alcohol consumption |
2.98 (1.19, 10.03) |
| Ninkron et al (2022)34 |
Thailand |
15-18 |
Cross-sectional |
290 |
Self-report |
Cigarette (51.5%) |
Parents deceased |
2.28 (1.21, 3.40) |
Strong |
| Divorced parents |
1.60 (1.15, 2.50) |
| Poor academic level |
2.50 (1.13, 3.55) |
| More money available |
1.19 (1.05, 1.34) |
| Severe depressive symptoms |
1.12 (1.07, 1.18) |
| Living with smokers |
3.78 (1.69, 8.07) |
| Alcohol consumption |
2.98 (1.19, 10.03) |
|
Lower-middle-income countries
|
| Odukoya et al (2016)35 |
Nigeria |
15-24 |
Cross-sectional |
326 |
Self-report |
Cigarette (32.5%)
Chewing tobacco (21.4%) |
Living with friends |
1.98 (1.01, 3.86) |
Strong |
| Alcohol drinking |
6.16 (3.03, 12.54) |
| Gender (male) |
2.56 (1.83, 7.80) |
| Lalithambigai et al (2016)36 |
India |
18-20 |
Cross-sectional |
720 |
Self-report |
Cigarette (20.4%) |
Male gender |
8.50 (3.26, 22.50) |
Moderate |
| Peer’s smoking |
5.15 (2.21, 11.90) |
| Daily pocket money |
4.16 (1.76, 9.82) |
| Bigwanto et al (2017)37 |
Indonesia |
15-19 |
Cross-sectional |
690 |
Self-report |
Cigarette (29.6%) |
Gender (male) |
31.80 (17.57, 57.63) |
Strong |
| Cigarette advertising |
1.24 (0.89, 1.73) |
| Availability |
3.72 (2.62, 5.28) |
| Kristina et al (2020)38 |
Indonesia |
16-24 |
Cross-sectional |
920 |
Self-report |
E-cigarette (10.68%)
Cigarette (57.61%) |
Gender (male) |
2.32 (1.23, 3.45) |
Strong |
| Alcohol consumption |
2.35 (1.56, 3.89) |
| Poor smoking knowledge |
1.92 (1.32, 3.22) |
| Smoking attitudes (Neutral) |
1.87 (1.31, 3.15) |
| Fauzi andAreesantichai (2020)39 |
Indonesia |
15-19 |
Cross-sectional |
1,318 |
Self-report |
E-cigarette (36.3%) |
Gender (male) |
3.52 (2.31, 5.35) |
Strong |
| Peer’s use of e-cigarette |
2.07 (1.31, 3.27) |
| Easy availability |
2.37 (1.52, 3.67) |
| School location |
1.71 (1.15, 2.50) |
| Tucktuck et al (2017)40 |
Palestine (west bank and Gaza strip |
18-24 |
Cross-sectional |
1,891 |
Self-report |
Waterpipe (24.4%) Cigarette (18.0%) |
Male gender |
10.91 (7.20, 16.40) |
Moderate |
| Rural areas |
1.90 (1.17, 3.00) |
| Living without family |
1.70 (1.19, 2.68) |
| High financial status |
1.60 (1.24, 2.20) |
| Low academic achievement |
4.50 (2.78, 7.30) |
| Baheiraei et al (2016)41 |
Iran |
15-18 |
Cross-sectional |
870 |
Self-report |
Cigarette (20.3%) |
Availability of tobacco |
2.90 (1.90, 4.20) |
Strong |
| Friends’ use of drugs |
3.40 (2.00, 6.00) |
| Intention to use tobacco |
2.60 (1.40, 4.70) |
| Interaction with antisocial peers |
3.40 (1.30, 8.70) |
| Poor family support |
2.30 (1.60, 3.30) |
| Family conflict |
1.80 (1.20, 2.60) |
| Academic failure |
3.00 (2.10, 4.20) |
| Efendi et al (2021)42 |
Indonesia |
15-24 |
Cross-sectional |
4,811 |
Self-report |
Cigarette (54.6%) |
Low educational level |
1.93 (1.52, 2.45) |
Strong |
| Exposure to tobacco by radio |
1.28 (1.12, 1.48) |
| Age 20-24 years |
2.80 (2.40, 3.20) |
| Grover et al (2020)43 |
India |
15-24 |
Cross-sectional |
13,329 |
Self-report |
Cigarette (5.0%)
Smokeless (10.9%) |
Residence (rural) |
1.30 (1.20, 1.54) |
Moderate |
| Unmarried |
1.50 (1.37, 1.70) |
| Akhter et al (2018)44 |
Pakistan |
18-24 |
Cross-sectional |
689 |
Self-report |
Cigarette (13.72%)
Waterpipe (49.01%) |
Social gatherings |
5.03 (1.18, 21.40) |
Moderate |
| Reduce stress wants to relax |
1.72 (1.03, 2.86) |
| No anti-smoking awareness on social media |
2.22 (1.24, 3.99) |
| Rahman and Tareque, 202045 |
Bangladesh |
15-24 |
Cross-sectional |
385 |
Self-report |
Cigarette (40.3%) |
Low monthly income |
7.97 (1.68, 37.70) |
Strong |
| Father’s smoking |
2.5 (1.39, 4.50) |
| Brother’s smoking |
2.88 (1.39, 5.96) |
| Friend’s smoking |
9.85 (5.85, 15.27) |
|
Low-income countries
|
| Duko et al (2019)46 |
Ethiopia |
15-22 |
Cross-sectional |
564 |
Self-report |
Cigarette (11.0 %) |
Friends’ smoke |
4.00 (2.04, 7.40) |
Strong |
| Alcohol drinking |
4.10 (1.84, 9.70) |
| Illicit drug use |
5.80 (1.90, 17.30) |
| Kubas and Wadi (2015)47 |
Yemen |
18-24 |
Cross-sectional |
480 |
Self-report |
Cigarette (2.4%)
water pipe (78.6%) |
Curiosity |
4.8% |
Week |
| Friends’ smoking |
9.5% |
| Enjoyment |
14.3% |
| Life stress |
9.5% |
Note. OR: Odds ratio; CI: Confidence interval.
Quality appraisal assessment
The authors systematically assessed the methodological quality of all 20 eligible studies using the Joanna Briggs Institute Meta-Analysis Assessment and Review Instrument.48 Critical appraisal tools for cross-sectional studies were used to evaluate the methodological quality of eligible studies. This tool covers eight components, including the study objectives, inclusion criteria, information about study participants and setting, measurement quality, identification and management of potential confounding variables, and statistical analyses. First, the eight components were rated on a three-point scale (1 = strong, 2 = moderate, or 3 = weak) based on the defined quality rating criteria.49 An overall “strong” rating was defined as having no weak and at least six strong ratings. An overall “moderate” rating was described as one weak and less than six strong ratings. A “weak” rating was warranted if two or more weak ratings were across the eight evaluation components.48
Results
Out of the 2,892 articles identified, 20 met the study eligibility criteria. Studies included in the review used a cross-sectional design. The average age (M ± standard deviation) was 19.45 ± 1.686. The sample size ranged from 290 to 13,329 (M = 2,054). The majority of studies were conducted in lower-middle-income countries (n = 11), followed by upper-middle-income countries (n = 7) and low-income countries (n = 2)
According to the quality appraisal evaluation (Figure 2), out of the eligible studies, fourteen28,30-35,37-39,41,42,45,47 were rated as strong, while five29,36,40,43,44 were rated as moderate in methodological rigor. Therefore, many studies had sound research designs and methodologies, which can lead to dependable and valid outcomes. However, one study46 received a weak rating, revealing areas where their methodologies could be enhanced to boost their overall quality and dependability.
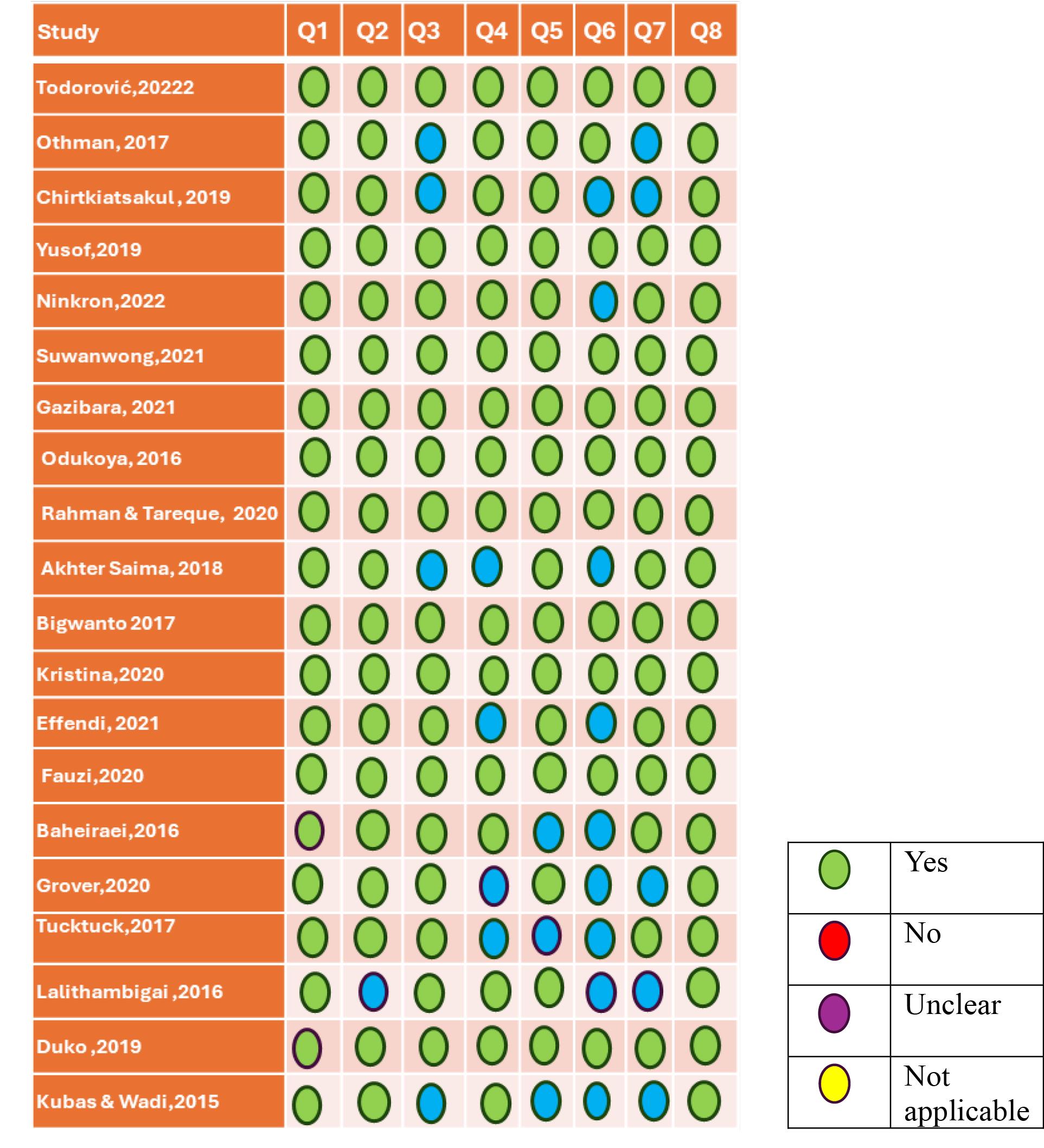
Figure 2.
JBI Checklist for the Quality Assessment of Cross-sectional Studies.
Q1. Were the criteria for inclusion in the sample clearly defined?
Q2. Were the study subjects and the setting described in detail?
Q3. Was the exposure measured in a valid and reliable way?
Q4. Were objective, standard criteria used for the measurement of the condition?
Q5. Were confounding factors identified?
Q6. Were strategies to deal with confounding factors stated?
Q7. Were the outcomes measured in a valid and reliable way?
Q8. Was the applied statistical analysis appropriate?
.
JBI Checklist for the Quality Assessment of Cross-sectional Studies.
Q1. Were the criteria for inclusion in the sample clearly defined?
Q2. Were the study subjects and the setting described in detail?
Q3. Was the exposure measured in a valid and reliable way?
Q4. Were objective, standard criteria used for the measurement of the condition?
Q5. Were confounding factors identified?
Q6. Were strategies to deal with confounding factors stated?
Q7. Were the outcomes measured in a valid and reliable way?
Q8. Was the applied statistical analysis appropriate?
Measurement and prevalence of youth tobacco use
All studies employed self-reporting techniques to evaluate current tobacco consumption. In upper-middle-income countries, tobacco smoking rates ranged from 6.4% to 51.5%, with different modes of consumption, such as cigarette smoking, e-cigarettes, and water pipe use.28-34 Meanwhile, tobacco use in lower-middle-income countries35-45 fluctuated between 5.0% and 57.6%, with various forms of consumption, such as cigarette smoking, e-cigarettes, water pipe use, smokeless tobacco, and chewing tobacco. Among youth in low-income countries,46,47 cigarette smoking ranged from 2.4% to 11.0%, with water pipe use being the most prevalent at 78.6%.
The main findings reported on the theory of triadic influence
Across all included studies, the most reported influences were on individual- (n = 18) and social- (n = 13) level factors, and fewer studies measured environmental-level factors (n = 10). The main findings are outlined in Table 2 and discussed later, according to the country’s level.
Table 2.
Summary of factors influencing tobacco use among youth based on the theory of triadic influence
|
Individual-level factors
|
|
a. Demographic
|
| Gender (Male) |
| Age |
| Unmarried |
| Living without family |
|
b. Economic factors
|
Low monthly income
Financial status (High)
Daily pocket money |
|
c. Psychological factors
|
Coping stress
Curiosity
Depression symptoms
Intention to tobacco use
Enjoyment |
|
d. Attitude and knowledge
|
Low education level
Favorable attitude toward smoking
Equivocal attitude |
|
e. Individual behavior
|
Alcohol consumption
Illicit drug use |
|
Social level factors
|
|
a. Parents education
|
|
Mothers with primary education
|
|
b. Family member’s tobacco use
|
Father smoking
Mother smoking
Brother smoking |
|
c. Stressful life events
|
Death of parents
Divorce of parents
Poor academic performance
Life stress
Poor family support
Family conflict |
|
d. Social networks
|
Social gathering
Peers smoking
Living with friends
Interaction with antisocial peers |
|
Environmental-level factors
|
|
a. secondhand smoke exposure
|
Secondhand smoke at home, public transport, and
living in a smoker’s environment |
|
b. Community context
|
Rural area
School location |
|
c. Media channels
|
Smoking advertising
Exposure to tobacco by radio |
|
d. Access of tobacco
|
| Easy availability |
Factors influencing tobacco use in upper-middle-income countries
Individual-level factors: This included demographics, economic status, psychological parameters, attitudes, and knowledge, as well as individual behavioral factors; four studies28-31 revealed that males are more prone to tobacco use than females. One study32 demonstrated that the high availability of money was also a significant factor in tobacco use. The findings of another study33 showed severe depressive symptoms, and one study29 showed that favorable or equivocal attitudes were positively associated with tobacco use. Three studies28,30,33 found that alcohol consumption and other illicit drugs increased the likelihood of tobacco use among youth.
Social-level factors: They consisted of parents’ education, peers’ tobacco use, and stressful life events. One study29 revealed that mothers with primary-level education increased the likelihood of tobacco use among youth. Another study31 indicated that the use of electronic cigarettes by peers increased the likelihood of tobacco use among youth.Further, one34 showed poor academic performance, and another34 indicated that family circumstances, such as divorced parents and the death of one or both parents, increased the likelihood of tobacco use.
Environmental factors: Three studies30,32,33 reported that secondhand smoke exposure is linked to higher rates of tobacco use among youth across various settings such as homes, restaurants, schools, public transport, or living with smokers.
Factors influencing tobacco use in lower-middle-income countries
Individual factors. Various demographic, economic, psychological, attitude and knowledge, and individual behavioral factors were found to be positively correlated with tobacco use among youth. These factors were included in six studies35-40 on gender (male), three studies40-42 on low education level, and three studies40,43,44 that have shown that unmarried individuals and those living away from their families may have fewer social constraints and are more likely to engage in tobacco. One study45 revealed low monthly income, and two studies36,40 showed that high financial status significantly increased the likelihood of tobacco use. One study38 demonstrated poor knowledge and neutral attitudes about smoking harm. Further, another study44 reported relaxation and coping with stress. Moreover, two studies38,44 showed that they intended to use tobacco and alcohol.
Social-level factors: They included family members smoking, stressful life events, and social networking.One study45 indicated that father and brother’s tobacco smoking was associated with tobacco use among youths. Further, another study41 indicated that family conflict and poor family support also increase the likelihood of tobacco smoking. Four studies36,39,41,45 represented that peer tobacco smoking and other illicit drug use were associated with tobacco use among youth. Additionally, three studies demonstrated that interaction with antisocial peers,41 living with friends,35 and social gatherings44 among youth had a positive association with tobacco use.
Environmental-level factors: They encompassed media channels, community context, and access to tobacco. Two studies revealed that exposure to tobacco smoking by radio42 and smoking advertising37 increases tobacco use. In contrast, one study44 reported that a lack of anti-smoking information on social media and traditional media is associated with its use among youth. Moreover, other studies showed that exposure to smoking in school locations41 and living in rural areas40,43 increased the likelihood of tobacco consumption among youth. Furthermore, three studies37,39,41 found that the easy availability of tobacco in markets and communities increased the likelihood of tobacco use among youth.
Factors influencing tobacco use in low-income countries
Individual-level factors: They consisted of psychological and behavioral parameters. One study47 indicated that curiosity and enjoyment were significantly associated with tobacco smoking among youth. Additionally, a study46 confirmed that the use of illegal drugs and alcohol consumption increased the likelihood of tobacco smoking among youths.
Social-level factors: They included social networks and stressful life events.Two studies46,47 reported that tobacco-smoking friends played an important role in tobacco use among youth. One study47 revealed that life stress was significantly associated with tobacco smoking among youth.
Discussion
This systematic review explored factors influencing tobacco use among youth in low-, lower-, and upper-middle-income countries. The review included 20 studies after narrowing down potentially relevant studies for the full text and considering the inclusion criteria. All included studies used cross-sectional designs that met the eligibility criteria for the review. The overall study quality varied from weak to strong. The primary factors that compromised methodological rigor were approaches utilized to address the confounding factors. Addressing potential confounding factors can be achieved using restriction, matching, and statistical adjustment methods.50 For instance, when investigating the correlation between factors influencing youth tobacco use, validity can be improved by limiting the study population, matching participants with similar characteristics, and employing statistical techniques such as regression to manage confounding variables.48 There was variation in the prevalence of tobacco use among different income categories of countries, with higher rates observed in lower-middle-income countries.
Studies included in the review investigated factors associated with three identified domains, namely, individual-, social-, and environmental-level factors. One individual-level factor was demographics. Male gender was identified as a significant influencing factor in lower- and upper-middle-income countries.28-31,35-40 According to the global gender gap report 2022,51 men globally show a lower healthy life expectancy than women, apart from Sub-Saharan Africa. Furthermore, men are at a higher risk of mortality due to non-communicable diseases, such as cardiovascular diseases, cancers, respiratory diseases, and diabetes, than women. Therefore, it is suggested that health policies and programs that consider the unique needs and preferences of both men and women be promoted and implemented in the future.
Socioeconomic status
There was an inconsistent relationship between financial status and tobacco use among youth in lower-middle-income countries. In two studies,36,40 higher income or daily pocket money was associated with increased tobacco use, whereas one study45 found that lower income was also significant. This may reflect the various levels of affordability and accessibility of tobacco products in different settings and the different motivations and influences of tobacco use among youth.
Psychological and behavioral factors
Studies29,41,47 conducted in low-income, lower-income, and upper-middle-income countries proved a positive association between favorable attitude, intention, and curiosity toward tobacco use. Earlier systematic reviews and meta-analyses revealed a positive association between favorable attitudes, intentions, and curiosity toward tobacco use among adolescents.52 Furthermore, studies44,47 from low- and lower-middle-income countries demonstrated that stress coping levels and relaxation had a significant relationship with tobacco use among youth. These findings underscore the importance of implementing comprehensive programs focusing on tobacco prevention and providing youth with effective stress-coping mechanisms and relaxation skills. In addition, regarding substance use, one study from low-income countries and another from upper-middle-income countries confirmed a positive association between tobacco use and individuals who were already consuming alcohol and using other illicit drugs.28,47 In an earlier review of a multi-country analysis, tobacco use was found to be influenced by alcohol consumption and other illicit drug use.53 This study indicated an explicit relationship between tobacco consumption, alcohol consumption, and other illicit drug use in low- and middle-income countries.
Social factors
Family impacts are essential components of the tobacco use behavior of youth.54 This study explicitly identified a significant relationship between tobacco use and factors influencing father and brother’s tobacco use and family conflicts in lower-middle-income countries.45 In comparison, a previous systematic review consistent with 41 studies in 20 low- and middle-income countries represented compelling evidence of an association between parental and sibling tobacco smoking and tobacco use among youths. Furthermore, the study also indicated that family conflicts, low parental monitoring, and poor parent-child communication are factors that affect youth tobacco use.55 Moreover, one study in an upper-middle-income country found that the lower education of mothers significantly increased the likelihood of tobacco use among youth.29 A previous review of education and tobacco use suggested that education may reduce tobacco consumption.55 Peer influence on tobacco use and other types of illicit drug use among youth was significant in two low-income countries46,47 and four lower-middle-income countries.36,39,41,45 Similarly, one study showed that peer tobacco use has a positive relationship with youth tobacco use.53
Environmental factors
Two studies42,44 conducted in lower-middle-income countries revealed that not using social media and traditional media, such as newspapers or television, and a lack of awareness about the harms of tobacco were positively associated with tobacco use. In contrast, an earlier survey performed among adolescents in 10 low-income countries in Africa and Asia has proven a positive correlation between tobacco use and exposure to tobacco advertising and promotion across multiple mass media platforms. Another study showed a negative correlation between tobacco use and awareness of the detrimental effects of tobacco use, as well as exposure to mass media anti-tobacco messages.56
It is essential to acknowledge the limitations of this systematic review when interpreting the findings. The major limitation of this study is the need for more generalizability on the youth of high-income countries because the studies consisted of only low-income, lower-income, and upper-middle-income countries. In addition, publication bias may occur due to the study period being limited between 2015 and 2023, which excludes studies published before this time limit. Furthermore, studies were excluded based on the definition of youth age. However, it is essential to consider the limitations of the studies with moderate and weak ratings, as they may have flaws in their methods or analyses.
This systematic review suggests that tobacco education programs should focus on mothers’ education levels. Further, it is important to address individual-, social-, and environmental-level factors such as male gender and psychological issues, as well as the influence of social networks, including peers, across various settings. Tailored interventions such as peer support, social norm change, and awareness campaigns that adhere to strict marketing regulations through social and traditional media should be explored for their effectiveness.
Highlights
-
This review analyzed 20 cross-sectional studies focusing on factors associated with youth tobacco use in low-income, lower-middle-income, and upper-middle-income countries.
-
Three overarching domains emerged based on the theory of the triadic influence model, namely, Individual-, social-, and environmental-level factors.
-
Individual-level factors included demographic, economic, psychological, attitude, knowledge, and individual behavioral factors.
-
Social-level factors were parental education, family member tobacco use, stressful life events, and social networks.
-
Environmental-level factors encompassed secondhand smoke exposure, community context, media channels, and access to tobacco.
Conclusion
The findings are categorized into individual, social, and environmental domains. Individual-level factors include demographic, economic, psychological, attitude and knowledge, and individual behavioral factors. Social-level factors encompass parental education, family member tobacco use, stressful life events, and social networks. Environmental factors include secondhand smoke exposure, community context, media channels, and access to tobacco. These factors were found to be significantly associated with tobacco use among youth in low-, lower-, and upper-middle-income countries. Consequently, it is imperative to implement targeted, tailored health interventions that aim to reduce tobacco use among individuals in diverse socioeconomic contexts.
Acknowledgments
This systematic review is part of a Ph.D. nursing dissertation submitted by Fahad Ali, supported by the Graduate ASEAN Non-ASEAN Countries Scholarship program at the Faculty of Nursing, Chulalongkorn University in Bangkok, Thailand.
Authors’ Contribution
Conceptualization: Fahad Ali Mangrio.
Data curation: Fahad Ali Mangrio, Suwimon Rojnawee.
Formal analysis: Fahad Ali Mangrio, Suwimon Rojnawee.
Funding acquisition: Penpaktr Uthis.
Investigation: Fahad Ali Mangrio, Suwimon Rojnawee.
Methodology: Penpaktr Uthis, Fahad Ali Mangrio.
Project administration: Penpaktr Uthis.
Resources: Penpaktr Uthis.
Software: Fahad Ali Mangrio.
Supervision: Penpaktr Uthis.
Validation: Fahad Ali Mangrio, Penpaktr Uthis.
Visualization: Fahad Ali Mangrio, Suwimon Rojnawee.
Writing–original draft: Fahad Ali Mangrio.
Writing–review & editing: Fahad Ali Mangrio, Suwimon Rojnawee.
Competing Interests
The authors have no conflict of interests to declare for this study.
Ethical Approval
This study included no human participants, and no ethical review was performed for it
Funding
This research received no external funding.
References
- Xi B, Liang Y, Liu Y, Yan Y, Zhao M, Ma C. Tobacco use and second-hand smoke exposure in young adolescents aged 12-15 years: data from 68 low-income and middle-income countries. Lancet Glob Health 2016; 4(11):e795-805. doi: 10.1016/s2214-109x(16)30187-5 [Crossref] [ Google Scholar]
- Al-Ibrahim MS, Gross JY. Tobacco use. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. Boston: Butterworths; 1990.
- World Health Organization (WHO). Tobacco. Geneva: WHO; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/tobacco. Updated July 31, 2023. Accessed September 15, 2023.
- World Health Organization (WHO). WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies. Geneva: WHO; 2017.
- Nazir MA, Al-Ansari A, Abbasi N, Almas K. Global prevalence of tobacco use in adolescents and its adverse oral health consequences. Open Access Maced J Med Sci 2019; 7(21):3659-66. doi: 10.3889/oamjms.2019.542 [Crossref] [ Google Scholar]
- Australian Institute of Health and Welfare (AIHW). National Drug Strategy Household Survey 2019. Canberra: AIHW; 2020.
- Leta K, Lauwerier E, Willems S, Vermeersch S, Demeester B, Verloigne M. Smoking prevention within social work organizations: a qualitative study about youngsters’ and youth workers’ perceptions. Health Promot Int 2023; 38(3):daad047. doi: 10.1093/heapro/daad047 [Crossref] [ Google Scholar]
- Stone E, Peters M. Young low and middle-income country (LMIC) smokers-implications for global tobacco control. Transl Lung Cancer Res 2017; 6(Suppl 1):S44-6. doi: 10.21037/tlcr.2017.10.11 [Crossref] [ Google Scholar]
- Akbar UU, Sari YP, Marta J, Satria D, Adry MR, Putri DZ, et al. Does tobacco consumption affect allocation of household expenditure: a study literature. In: Proceedings of the Sixth Padang International Conference on Economics Education, Economics, Business and Management, Accounting and Entrepreneurship (PICEEBA 2020). Atlantis Press; 2021.
- Drope J. Tobacco Growing and the Environment: An Unfolding Global Disaster. National Cancer Institute; 2022. Available from: https://www.cancer.gov/about-nci/organization/cgh/blog/2022/worldnotobaccoday2022. Updated May 27, 2022. Accessed November 10, 2023.
- Hamadeh N, Van Rompaey C, Metreau E. World Bank Group Country Classifications by Income Level for FY24 (July 1, 2023- June 30, 2024). Washington, DC: World Bank Group; 2023.
- World Bank. The World by Income and Region. Washington, DC: World Bank; 2022. Available from: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html.
- Nawi AM, Ismail R, Ibrahim F, Hassan MR, Abdul Manaf MR, Amit N. Risk and protective factors of drug abuse among adolescents: a systematic review. BMC Public Health 2021; 21(1):2088. doi: 10.1186/s12889-021-11906-2 [Crossref] [ Google Scholar]
- Centers for Disease Control and Prevention (CDC). Preventing Tobacco Use Among Youth and Young Adults: A Report of the Surgeon General. Atlanta, GA: CDC; 2012.
- American Lung Association. Tobacco Use Among Children and Teens. Chicago, Illinois: American Lung Association; 2023. Available from: https://www.lung.org/quit-smoking/smoking-facts/tobacco-use-among-children. Updated May 31, 2022. Accessed September 15, 2023.
- Fanshawe TR, Halliwell W, Lindson N, Aveyard P, Livingstone-Banks J, Hartmann-Boyce J. Tobacco cessation interventions for young people. Cochrane Database Syst Rev 2017; 11(11):CD003289. doi: 10.1002/14651858.CD003289.pub6 [Crossref] [ Google Scholar]
- Linetzky B, Mejia R, Ferrante D, De Maio FG, Diez Roux AV. Socioeconomic status and tobacco consumption among adolescents: a multilevel analysis of Argentina’s Global Youth Tobacco Survey. Nicotine Tob Res 2012; 14(9):1092-9. doi: 10.1093/ntr/nts004 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg 2021; 88:105906. doi: 10.1016/j.ijsu.2021.105906 [Crossref] [ Google Scholar]
- Sawyer SM, Afifi RA, Bearinger LH, Blakemore SJ, Dick B, Ezeh AC. Adolescence: a foundation for future health. Lancet 2012; 379(9826):1630-40. doi: 10.1016/s0140-6736(12)60072-5 [Crossref] [ Google Scholar]
- United Nations. World Population Prospects 2019: Department of Economic and Social Affairs Youth. New York: United Nations; 2019.
- Xu C, Ju K, Lin L, Jia P, Kwong JS, Syed A. Rapid evidence synthesis approach for limits on the search date: how rapid could it be?. Res Synth Methods 2022; 13(1):68-76. doi: 10.1002/jrsm.1525 [Crossref] [ Google Scholar]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015; 4(1):1. doi: 10.1186/2046-4053-4-1 [Crossref] [ Google Scholar]
- Helbach J, Pieper D, Mathes T, Rombey T, Zeeb H, Allers K. Restrictions and their reporting in systematic reviews of effectiveness: an observational study. BMC Med Res Methodol 2022; 22(1):230. doi: 10.1186/s12874-022-01710-w [Crossref] [ Google Scholar]
- Pinheiro C, Krishnaveni A, Thuruthiyath LR. Tobacco use and its determinants among school going adolescents. J Evol Med Dent Sci 2022; 11(7):684-9. doi: 10.14260/jemds.v11i7.146 [Crossref] [ Google Scholar]
- Garrard J. Health Sciences Literature Review Made Easy. 6th ed. Jones & Bartlett Learning; 2022.
- Cumpston MS, McKenzie JE, Welch VA, Brennan SE. Strengthening systematic reviews in public health: guidance in the Cochrane Handbook for Systematic Reviews of Interventions, 2nd edition. J Public Health (Oxf) 2022; 44(4):e588-92. doi: 10.1093/pubmed/fdac036 [Crossref] [ Google Scholar]
- Flay BR, Snyder FJ, Petraitis J. The theory of triadic influence. In: Emerging Theories in Health Promotion Practice and Research. 2nd ed. Hoboken, NJ: Jossey-Bass; 2009.
- Othman N, Kasem AO, Salih FA. Waterpipe smoking among university students in Sulaimaniyah, Iraqi Kurdistan: prevalence, attitudes, and associated factors. Tanaffos 2017; 16(3):225-32. [ Google Scholar]
- Chirtkiatsakul B, Jani R, Kadir RA, Nordin AS, Azizi R. Prevalence of and factors associated with smoking among University of Malaya students in Malaysia. Southeast Asian J Trop Med Public Health 2019; 50(6):1202-11. [ Google Scholar]
- Suwanwong C, Kalapat R, Pitayarangsarit S, Chaiyasong S. Factors related to adolescent smoking: a nationally representative cross-sectional study in Thailand. Open Access Maced J Med Sci 2021; 9:1267-72. doi: 10.3889/oamjms.2021.7453 [Crossref] [ Google Scholar]
- Yusof NA, Zin FM, Idris NS, Mohammad R. Alternative tobacco products use among late adolescents in Kelantan, Malaysia. Korean J Fam Med 2019; 40(4):254-60. doi: 10.4082/kjfm.18.0016 [Crossref] [ Google Scholar]
- Todorović I, Cheng F, Stojisavljević S, Marinković S, Kremenović S, Savić P. Prevalence of cigarette smoking and influence of associated factors among students of the University of Banja Luka: a cross-sectional study. Medicina (Kaunas) 2022; 58(4):502. doi: 10.3390/medicina58040502 [Crossref] [ Google Scholar]
- Gazibara T, Milic M, Parlic M, Stevanovic J, Mitic N, Maric G. What differs former, light and heavy smokers? Evidence from a post-conflict setting. Afr Health Sci 2021; 21(1):112-22. doi: 10.4314/ahs.v21i1.16 [Crossref] [ Google Scholar]
- Ninkron P, Yau S, Noosorn N. Predictors of smoking initiation among Thai adolescents from low-income backgrounds: a case study of Nakhon Pathom low-cost housing estates. Tob Induc Dis 2022; 20:21. doi: 10.18332/tid/145143 [Crossref] [ Google Scholar]
- Odukoya OO, Dada MR, Olubodun T, Igwilo UA, Ayo-Yusuf OA. Risk perception and correlates of tobacco use among young people outside of formal school settings in Lagos State, Nigeria. Asian Pac J Cancer Prev 2016; 17(6):2833-9. [ Google Scholar]
- Lalithambigai G, Rao A, Rajesh G, Ramya S, Pai BH. Predictors of cigarette smoking among young adults in Mangalore, India. Asian Pac J Cancer Prev 2016; 17(1):45-50. doi: 10.7314/apjcp.2016.17.1.45 [Crossref] [ Google Scholar]
- Bigwanto M, Mongkolcharti A, Peltzer K, Laosee O. Determinants of cigarette smoking among school adolescents on the island of Java, Indonesia. Int J Adolesc Med Health 2017; 29(2):20150036. doi: 10.1515/ijamh-2015-0036 [Crossref] [ Google Scholar]
- Kristina SA, Rosyidah KA, Ahsan A. Trend of electronic cigarette use among students in Indonesia. Int J Pharm Res 2020; 12(3):657-61. doi: 10.31838/ijpr/2020.12.03.099 [Crossref] [ Google Scholar]
- Fauzi R, Areesantichai C. Factors associated with electronic cigarettes use among adolescents in Jakarta, Indonesia. J Health Res 2022; 36(1):2-11. doi: 10.1108/jHR-01-2020-0008 [Crossref] [ Google Scholar]
- Tucktuck M, Ghandour R, Abu-Rmeileh NM. Waterpipe and cigarette tobacco smoking among Palestinian university students: a cross-sectional study. BMC Public Health 2017; 18(1):1. doi: 10.1186/s12889-017-4524-0 [Crossref] [ Google Scholar]
- Baheiraei A, Soltani F, Ebadi A, Rahimi Foroushani A, Cheraghi MA. Risk and protective profile of tobacco and alcohol use among Iranian adolescents: a population- based study. Int J Adolesc Med Health 2016;29(3). 10.1515/ijamh-2015-0089.
- Efendi F, Aidah FN, Has EMM, Lindayani L, Reisenhofer S. Determinants of smoking behavior among young males in rural Indonesia. Int J Adolesc Med Health 2019; 33(5):20190040. doi: 10.1515/ijamh-2019-0040 [Crossref] [ Google Scholar]
- Grover S, Anand T, Kishore J, Tripathy JP, Sinha DN. Tobacco use among the youth in India: evidence from Global Adult Tobacco Survey-2 (2016-2017). Tob Use Insights 2020; 13:1179173x20927397. doi: 10.1177/1179173x20927397 [Crossref] [ Google Scholar]
- Akhter S, Mustafa H, Warraich UA, Rizvi N. Frequency and factors associated with tobacco smoking among young female students in Pakistan. Khyber Med Univ J 2018; 10(2):76-80. doi: 10.35845/kmuj.2018.16812 [Crossref] [ Google Scholar]
- Rahman KM, Tareque MI. Determinants of cigarette/bidi smoking among youth male in rural Mymensingh of Bangladesh: a cross-sectional study. PLoS One 2020; 15(12):e0244335. doi: 10.1371/journal.pone.0244335 [Crossref] [ Google Scholar]
- Duko B, Melese Y, Ebrahim J. Determinants of cigarette smoking among adolescents in Ethiopia: a cross-sectional study. Tob Induc Dis 2019; 17:62. doi: 10.18332/tid/110800 [Crossref] [ Google Scholar]
- Kubas MA, Wadi M. Comparison of smoking and khat chewing habits between medical and non-medical female students at UST, Sana’a, Yemen. J Res Health Sci 2015; 15(4):262-5. [ Google Scholar]
- Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Chapter 3: systematic reviews of effectiveness. In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI; 2020. Available from: https://synthesismanual.jbi.global. Updated November 9, 2023. Accessed November 12, 2023.
- Joanna Briggs Institute (JBI). Checklist for Quasi-Experimental Studies. Australia: JBI; 2020. Available from: http://joannabriggs.org/research/critical-appraisal-tools.htmlwww.joannabriggs.org. Updated 2020. Accessed November 11, 2023.
- Smith C. Methods to Account for Confounding in Observational Studies. London: SAGE Publications; 2011.
- World Economic Forum (WEF). Global Gender Gap Report. Geneva: WEF; 2022. Available from: https://www.weforum.org/publications/global-gender-gap-report-2022/in-full/1-benchmarking-gender-gaps-2022/. Updated July 13, 2022. Accessed December 10, 2011.
- Barati M, Jormand H, Bashirian S, Doosti-Irani A, Rezapur-Shahkolai F. The role of media on the intention of adolescents smoking: a systematic review and meta-analysis. J Educ Community Health 2020; 7(4):311-23. doi: 10.29252/jech.7.4.311 [Crossref] [ Google Scholar]
- Mutumba M, Schulenberg JE. Tobacco and alcohol use among youth in low- and middle-income countries: a multi-country analysis on the influence of structural and micro-level factors. Subst Use Misuse 2019; 54(3):396-411. doi: 10.1080/10826084.2018.1497063 [Crossref] [ Google Scholar]
- Theilmann M, Lemp JM, Winkler V, Manne-Goehler J, Marcus ME, Probst C. Patterns of tobacco use in low- and middle-income countries by tobacco product and sociodemographic characteristics: nationally representative survey data from 82 countries. BMJ 2022; 378:e067582. doi: 10.1136/bmj-2021-067582 [Crossref] [ Google Scholar]
- Utku Özmen M. Causal effect of education on tobacco use in low- and-middle-income countries. Nicotine Tob Res 2023; 25(8):1474-80. doi: 10.1093/ntr/ntad056 [Crossref] [ Google Scholar]
- Brennan E, Jeong M, Momjian-Kybert A, Hornik R. Preventing and Reducing Tobacco Use among Youth and Young Adults: A Systematic Review of the Effectiveness of Mass Media Interventions, 2008-2013. CECCR/TCORS Working Paper Series. University of Pennsylvania; 2016. p. 1-70.