J Res Health Sci. 25(4):e00667.
doi: 10.34172/jrhs.11310
Original Article
Investigating the Risk Factors in Progression of HIV Disease Using an Illness-Death Multistate Model
Roghayyeh Hassanzadeh Conceptualization, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing, 1, 2 
Hossein Mahjub Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, 3
Mohammad Mirzaei Data curation, Writing – original draft, 4
Fariba Keramat Writing – original draft, 5, 6
Maryam Farhadian Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, 3, *
Author information:
1Department of Biostatistics, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
2Student Research Committee, Hamadan University of Medical Sciences, Hamadan, Iran
3Research Center for Health Sciences, Institute of Health Sciences and Technologies, Avicenna Health Research Institute, Hamadan University of Medical Sciences, Hamadan, Iran
4Department of Epidemiology, School of Public Health, Hamadan Health Center, Hamadan University of Medical Sciences, Hamadan, Iran
5Department of Infectious Diseases, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
6Brucellosis Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background:
The trend of human immunodeficiency virus (HIV) disease progress is different for every patient. Some patients may experience events during the course of their disease that can affect disease progression and death. The main objective of the present study was to investigate the effect of risk factors in progression of HIV disease, taking into account intermediate events, using a multistate model.
Study Design:
A retrospective cohort study.
Methods:
The current study used information from 673 HIV-infected adult patients registered at the Hamadan Provincial Health Center in Iran, between 1997 and 2023. A multistate framework was described to investigate the progression of HIV disease over time. Three states (HIV-infected, acquired immunodeficiency syndrome [AIDS], and death) and three possible transitions (from HIV to AIDS, from HIV to death, and from AIDS to death) were considered in this framework. An illness-death multistate model was applied to determine the effect of risk factors on these transitions.
Results:
The results revealed that receiving antiretroviral therapy (ART) significantly decreased the hazard of transition from HIV to AIDS, whereas older age, tuberculosis (TB) co-infection, and treatment with the final guideline intensified the hazard of the mentioned transition. Low education, older age, and unprotected sexual transmission increased the risk of transition from HIV to death, while receiving ART and treatment with the final guideline decreased the risk of this transition. Receiving ART, being employed, having a history of prison, and being treated with the final guideline could decrease the hazard of transition from AIDS to death, whereas TB co-infection increased the hazard of this transition.
Conclusion:
Implementing strategies for early diagnosis, timely treatment, adherence to treatment, as well as screening and TB treatment, especially at younger ages, can be useful in reducing AIDS progression and mortality.
Keywords: HIV/AIDS, Survival analysis, Multistate model, Antiretroviral therapy, Tuberculosis
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Hassanzadeh R, Mahjub H, Mirzaei M, Keramat F, Farhadian M. Investigating the risk factors in progression of HIV disease using an illness-death multistate model. J Res Health Sci. 2025; 25(4):e00667. doi:10.34172/jrhs.11310
Background
Despite significant progress in prevention and treatment, the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is still a major global public health concern. To date, around 88.4 million people have been infected with HIV, and around 42.3 million have died worldwide as a result of HIV. In 2023 alone, nearly 1.3 million people were infected with HIV, and 630,000 people died as a result of HIV.1 Despite global efforts to end the AIDS epidemic by 2030, the current rate of reduction is insufficient.2 As in other parts of the world, there are also many cases of HIV in Iran. According to the latest data from 2023, 42,000 adults were infected with the virus, 2,500 new cases were reported, and 1,900 died of AIDS.3
Although there is currently no definitive cure for HIV, prevention and control of the disease are possible with antiretroviral therapy (ART), a widely used medical treatment.1 Treatment with ART has been shown to significantly reduce viral replication while improving the performance of the immune system, thereby improving the quality of life and dramatically increasing life expectancy.4-6 It also plays a crucial role in HIV/AIDS prevention and can help slow down the progression of AIDS and reduce the risk of mortality.6-11 Without ART, most HIV-infected people develop AIDS within 5–10 years, and in some cases even faster, within only 3–5 years, and usually survive only 2–3 years after AIDS diagnosis.12,13
However, the progression of HIV disease in HIV-infected patients can vary due to immunological, genetic, environmental, and virological factors.14,15 The treatment process can also be complicated by some factors, including chronic conditions associated with immunodeficiency, chronic viral and bacterial infections, and HIV drug resistance.10,16-18 In addition, co-infection with opportunistic infections, such as tuberculosis (TB) and hepatitis, as well as poor adherence to treatment and self-medication due to drug-drug interactions, can increase the risk of death and AIDS.10,15,17,19-21 In this way, the disease can progress to AIDS in some people but not in others. Patients who progress to the AIDS stage have a higher risk of death, and it is important to identify the prognostic factors that influence a patient’s progression to AIDS. Moreover, the development of AIDS can alter the progression of HIV disease, and the effect of prognostic factors can be altered by AIDS. As a result, the effects of the variables on time to AIDS onset and time to death with and without AIDS may be different. Therefore, special statistical methods are required to determine the prognostic factors that influence the survival of these patients.
A HIV-positive patient may experience an intermediate event, such as progression to AIDS and then death, or may die without such progression.10,11,22 This is an important aspect that has often been neglected in many HIV/AIDS survival studies, and separate analyses have been conducted for each endpoint.16,23-25 In these analyses, the relationships between these events could not be taken into account. The neglect of intermediate states and their time of occurrence can also lead to biased or misleading results.10,11 A common approach to this problem is to use multistate models that model different types of events simultaneously. Multistate models describe the progression of the disease and the transitions between the different stages over time and provide a better understanding of the impact of prognostic factors on disease progression and outcomes.26-28 Therefore, this study aims to investigate the effect of risk factors on progression to AIDS and death, both with and without progression to AIDS, using an illness-death multistate model.
Methods
Data description
A retrospective cohort study was conducted using data from HIV-infected patients registered at the Hamadan Provincial Health Center in Iran between 1997 and 2023. The main dataset contained 730 patients who were at least 15 years old and had a confirmed diagnosis of HIV infection. In the present article, based on the multistate model, 57 patients who had AIDS at the time of study entry were excluded from the main dataset, and the analysis was performed on the remaining 673 patients.
A person with HIV infection was considered HIV positive, regardless of clinical stage, if confirmed by laboratory criteria according to the definitions and requirements of each country.30 In Iran, a person is considered HIV-positive if, until a few years ago, they had two positive enzyme-linked immunosorbent assay (ELISA) tests and a positive Western blot, or, more recently, a rapid HIV test followed by two positive ELISA tests, one of which is a fourth-generation test.31 In addition, according to the World Health Organization, an HIV case was considered an AIDS case if diagnosed with a stage 4 condition, either presumptive or definitive, and/or if their CD4 count dropped below 200 per mm³ of blood.30
Baseline demographic and clinical information was extracted from patients’ medical records using a predefined checklist, including gender (female/male), age ( ≤ 30, 31-40, 41–50, and > 50 years), marital status (married, single, and other), education level (high [high school to academic]/low [illiterate to middle school]), and occupational status (employed/unemployed). Other related data were the treatment guideline used (initial guideline, intermediate guideline, and final guideline), history of drug abuse (yes/no), history of imprisonment (yes/no), mode of HIV transmission (injecting drug user, unprotected sexual and unknown), ART status (yes/no), and TB infection (yes/no). Based on data registered by the Ministry of Health and Medical Education, we just specified the status of covariates at the time of HIV diagnosis.
The treatment guideline was defined using the variables according to the treatment guidelines in force at the time of HIV diagnosis: the initial guideline (before 2006), the intermediate guideline (2006–2011), and the final guideline (after 2011). The main differences between these guidelines concern the timing of ART initiation: the initial and intermediate guidelines recommended ART initiation based on specific CD4 cell counts, whereas the final guideline recommends ART initiation immediately after HIV diagnosis, regardless of CD4 count.
The study focused on two main endpoints: AIDS and death. The outcomes of interest were the times of entry into each state (in months), including time to AIDS progression, time to death (without AIDS progression), and time to death after AIDS progression. All patients who were alive at the end of the study were censored for the death endpoint, and those who did not progress to AIDS were also censored for the AIDS event. Additionally, patients who were lost to follow up or withdrew from the study were considered censored. The multistate structure of the data is illustrated in Figure 1.
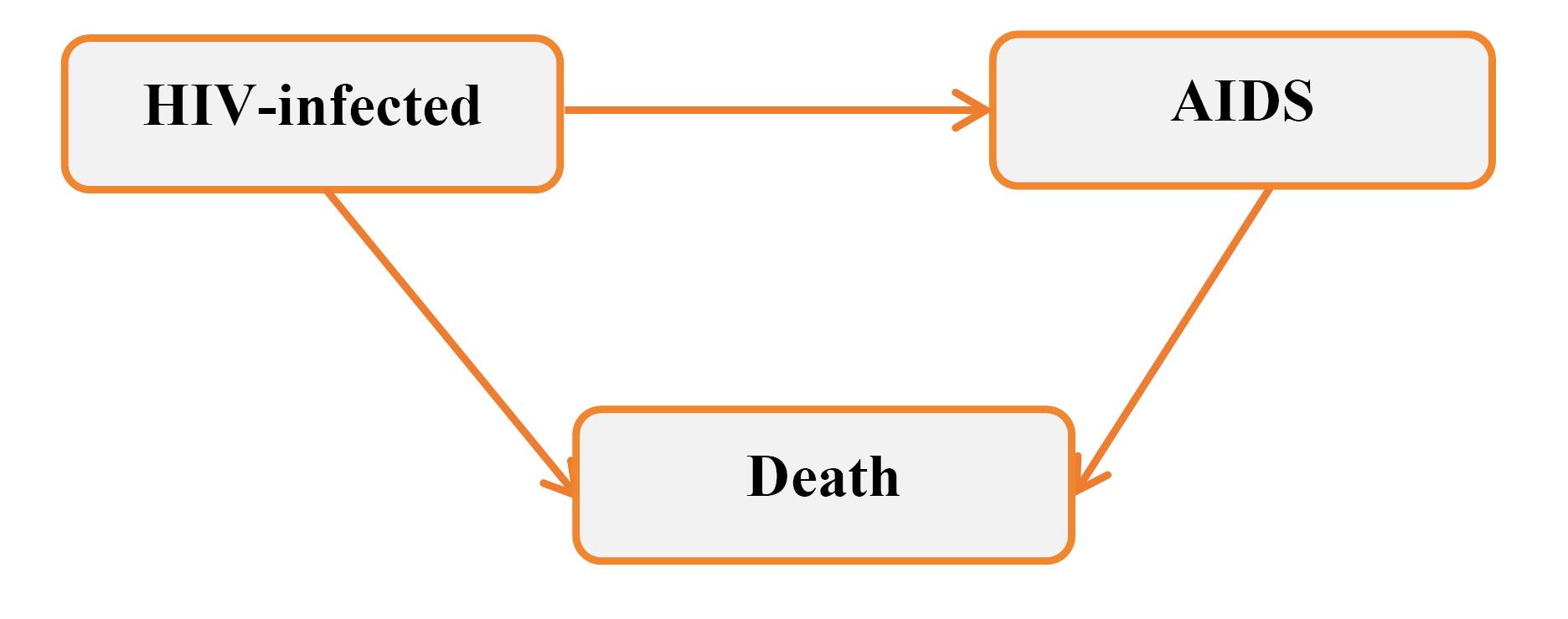
Figure 1.
The Multi-State Structure of HIV Patients. Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome
.
The Multi-State Structure of HIV Patients. Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome
Multistate model
Multistate models are used to describe the progression of disease over time using a set of states and transitions between them. In these models, different types of events (including final and intermediate events) are modeled simultaneously. Each model is defined by states and transitions. States represent the status of a subject at a given time, while transitions refer to the movement from one state to another. There are three different types of states (initial, transient, and absorbing). An initial state is the point at which a subject enters the process, and a transient state is a state that a subject can enter and exit at any time. An absorbing or final state is one that the subject cannot leave once it is entered. Unlike absorbing and initial states, transient states can be revisited multiple times during the course of the study. In these models, both transient and absorbing states can be considered outcomes, and each possible transition between states is treated as an event. Each possible transition is associated with a transition hazard, representing the instantaneous risk of moving from one state to another at a specific time. In multistate models, transition hazards, called transition intensities, are modeled, and the effects of covariates on them are assessed.26-28
An HIV-infected individual may experience death either after progression to AIDS or without developing AIDS. For this reason, in this study, the progression of HIV was described by incorporating an intermediate state (AIDS), and an illness-death multistate was considered with three states: HIV infection (the initial state), AIDS, and death (the absorbing state), and three transitions: from HIV infection to AIDS, from AIDS to death, and from HIV infection to death (Figure 1). A transition-specific Cox model was fitted to investigate the effects of covariates on these transition hazards. The Markov property is assumed, implying that the transition hazard at any given time depends solely on the individual’s current state rather than on their history. The mathematical definition of the model is as follows:
(1)
where λij,0 (t) is the baseline intensity function for the transition from state i to state j at time t. βij represents the vector of regression coefficients, and Zij denotes the vector of covariates specific to the transition from state i to state j.
Maximum likelihood estimation was used to estimate the regression coefficients of the model. Then, the effect of a covariate, such as Zij,p on the transition intensity of a specific transition
was measured using the hazard ratio, which is defined as exp (βij,p).
It should be noted that the Markov assumption was checked and confirmed. Further, to select the variables in the final model, a univariate analysis was applied, and a multistate model was fitted with a single variable. Next, the significance of each variable in all transitions was examined, and variables with a significance level less than 0.15 in at least one transition were included in the final multiple multistate models.
All analyses were performed using “Survival”, “mstate”, and “markovMSM” packages of R software (version 4.2.2), with a significant level of 0.05.
Results
Of the 673 HIV-positive patients, 536 (79.6%) were male and 137 (20.4%) were female, with an age range of 18–85 years. The mean age ( ± standard deviation) of participants at the time of diagnosis was 35.80 ( ± 9.48) years, and 405 (60.1%) of them were treated according to initial and intermediate guidelines. Among patients, 41.3% and 53.3% were married and unemployed, respectively. Further, 42.6% were in the 31–40 age group, and 66.7% were infected with HIV through injection drug use. Furthermore, 82.8% had a low level of education. Nearly half of the patients (n = 347, 51.6%) received no ART, and 73.8% of them died. A small number of patients (n = 42, 6.2%) had co-TB. In addition, most patients had a history of imprisonment (n = 427, 63.4%) and a history of drug abuse (n = 514, 76.4%). Further details of participant characteristics are provided in Table 1.
Table 1.
Demographic and clinical characteristics of HIV-infected patients in the total sample and event groups (AIDS and death) in Hamadan province
|
Variables
|
Total, n=673
|
AIDS, n=275
|
Death, n=329
|
Median survival time (month)
|
P
value
|
| Gender |
|
|
|
|
0.001 |
| Female |
137 |
65 |
26 |
- |
|
| Male |
536 |
210 |
303 |
90 |
|
| Age (year) |
|
|
|
|
0.005 |
| ≤ 30 |
210 |
85 |
118 |
105 |
|
| 31-40 |
287 |
125 |
127 |
151 |
|
| 41-50 |
124 |
44 |
65 |
73 |
|
| > 50 |
52 |
21 |
19 |
136 |
|
| Marital status |
|
|
|
|
0.004 |
| Married |
287 |
101 |
112 |
172 |
|
| Single |
239 |
101 |
146 |
80 |
|
| Other |
156 |
73 |
71 |
152 |
|
| Education |
|
|
|
|
0.056 |
| High (high school to academic) |
116 |
42 |
44 |
142 |
|
| Low (illiterate to middle school) |
557 |
233 |
285 |
105 |
|
| Occupational status |
|
|
|
|
0.227 |
| Employed |
314 |
115 |
142 |
119 |
|
| Unemployed |
359 |
160 |
187 |
110 |
|
| Drug abuse |
|
|
|
|
0.001 |
| No |
159 |
70 |
23 |
- |
|
| Yes |
514 |
205 |
306 |
87 |
|
| Imprisonment |
|
|
|
|
0.001 |
| No |
246 |
105 |
79 |
183 |
|
| Yes |
427 |
170 |
250 |
91 |
|
| Transmission way |
|
|
|
|
0.001 |
| Injecting drug user |
449 |
186 |
281 |
86 |
|
| Unprotected sexual |
184 |
73 |
40 |
- |
|
| Unknown |
40 |
16 |
8 |
- |
|
| Antiretroviral therapy |
|
|
|
|
0.001 |
| No |
347 |
74 |
256 |
52 |
|
| Yes |
326 |
201 |
73 |
- |
|
| Tuberculosis infection |
|
|
|
|
0.034 |
| No |
631 |
235 |
300 |
118 |
|
| Yes |
42 |
40 |
29 |
79 |
|
| Treatment guideline used |
|
|
|
|
0.001 |
| Initial guideline |
143 |
48 |
112 |
66 |
|
| Intermediate guideline |
262 |
123 |
159 |
99 |
|
| Final guideline |
268 |
104 |
58 |
- |
|
Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome.
The median follow-up time of the study was 69 months (interquartile range: 26–131.5). The mean and median survival times were 151.84 months and 112 months, respectively. Significant differences in survival were observed across the subgroups of all variables, except for occupational status and education (Log-rank test, Table 1).
Based on the multistate structure (Figure 1), the number of direct transitions observed between the defined states during the study period is presented in Table 2. Among the 673 HIV-positive patients entered in the initial state, 275 (40.9%) progressed to AIDS, 220 (32.7%) died without progressing to AIDS, and 178 (26.4%) were censored for both progression to AIDS and death. Of the 275 patients who developed AIDS, 109 (39.6%) died, and 166 (60.4%) were censored for death following progression to AIDS. In total, 329 (48.9%) patients died, and 344 (51.1%) were censored during the follow-up period.
Table 2.
Numbers of direct transitions between states during the study period in HIV-infected patients
|
From
|
To
|
(1) HIV-infected
|
(2) AIDS
|
(3) Death
|
Total entering
|
| (1) HIV-infected |
|
178 |
275 |
220 |
673 |
| (2) AIDS |
|
0 |
166 |
109 |
275 |
| (3) Death |
|
0 |
0 |
329 |
329 |
Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome.
The cumulative hazard for each transition over time is depicted in Figure 2. The hazard of transition from HIV to death was consistently lower than that of HIV to AIDS throughout the study period. The hazard of transition from AIDS to death was the highest within the first 10 years, after which the hazard of transition from HIV to AIDS was high until the end of the study. In addition, the stacked transition probability plot is illustratedin Figure 3. In this plot, the vertical distance between two adjacent curves represents the probability of patients being in a specific state at a given time point. For example, 150 months after HIV-infection, the estimated probabilities of being in the HIV, AIDS, and death states were 0.15, 0.30, and 0.55, respectively.
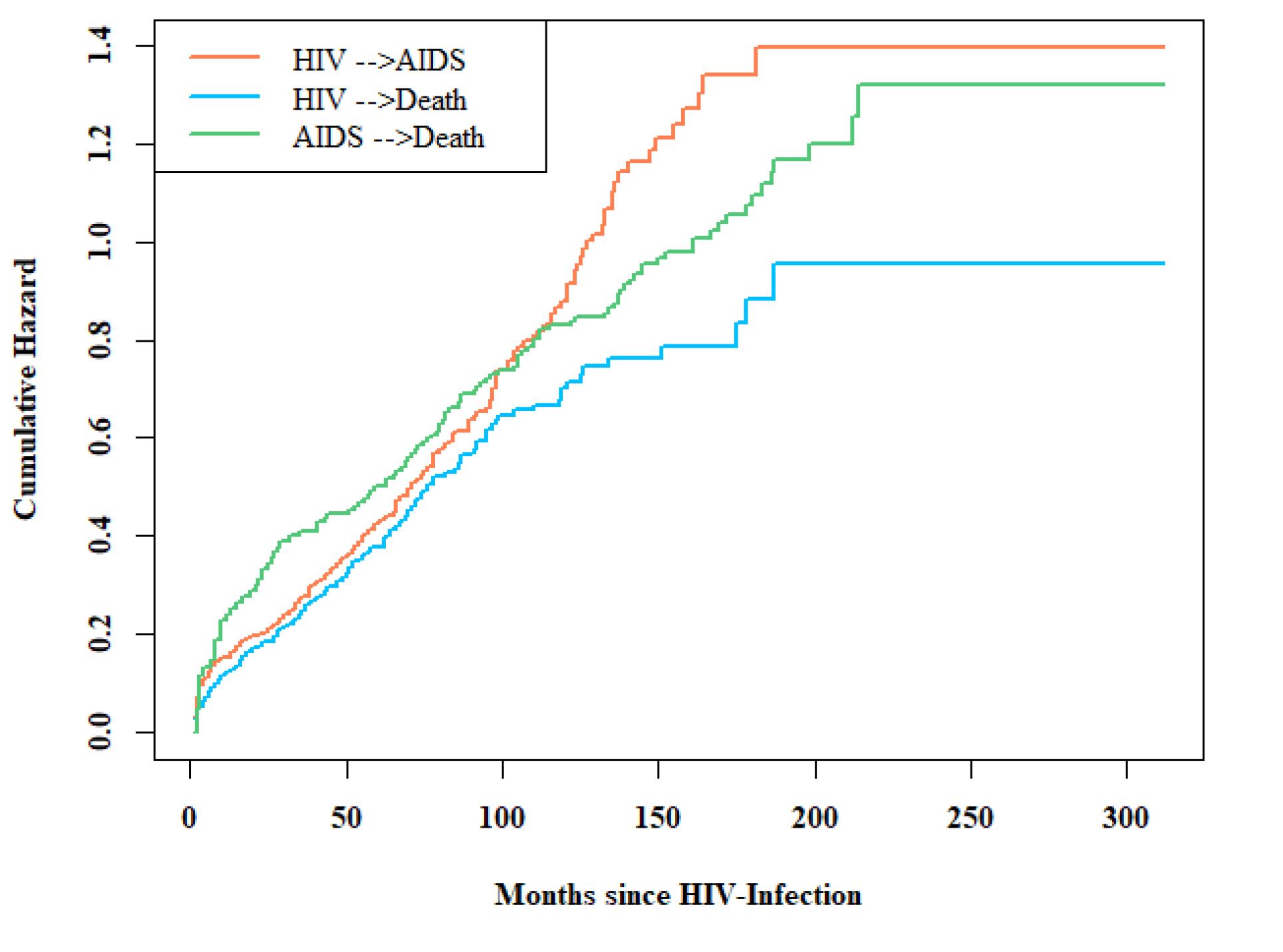
Figure 2.
Estimated cumulative hazards of transition from HIV to AIDS, from HIV to death, and from AIDS to death in the multistate model. Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome
.
Estimated cumulative hazards of transition from HIV to AIDS, from HIV to death, and from AIDS to death in the multistate model. Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome
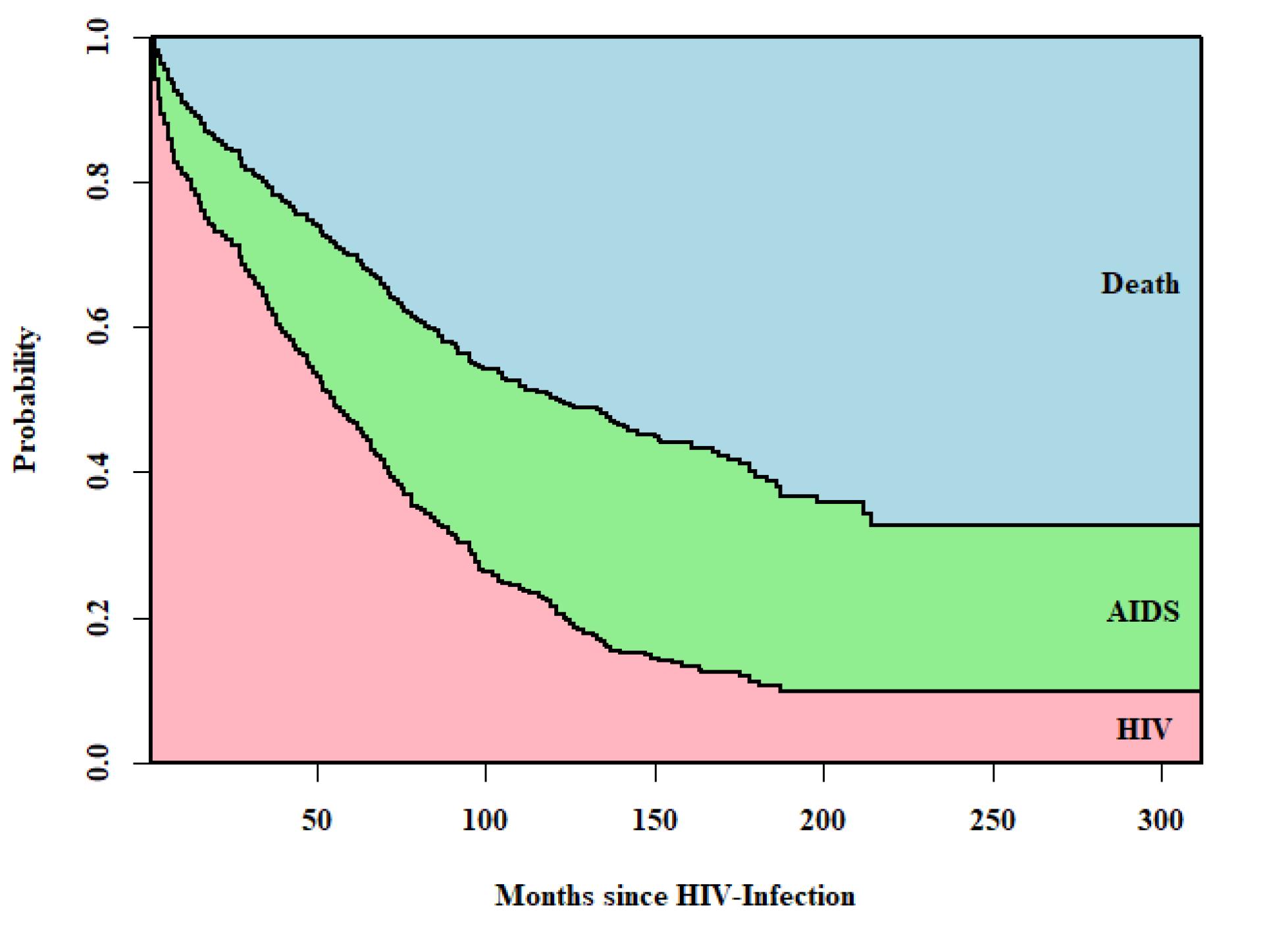
Figure 3.
Stacked transition probabilities for HIV-infected patients. Note. HIV: Human immunodeficiency virus
.
Stacked transition probabilities for HIV-infected patients. Note. HIV: Human immunodeficiency virus
The results of the illness-death multistate model are reported in Table 3, demonstrating the effects of different covariates on transition hazards. According to the results, both ART and the year of HIV diagnosis were significantly associated with the intensities of all three transitions. Specifically, HIV patients who received ART had a significantly lower risk of both progression to AIDS (hazard ratio [HR] = 0.43, P < 0.001) and direct transition to death (HR = 0.05, P < 0.001) than those who did not receive ART. Additionally, among patients who progressed to AIDS, those who received ART had a lower risk of death (HR = 0.38, P < 0.001). Moreover, patients treated under the final guideline had a significantly higher risk of progression to AIDS (HR = 1.95, P < 0.001) compared to those treated under the initial guideline, but a lower risk of direct transition to death (HR = 0.55, P = 0.041). In patients who progressed to AIDS, patients treated with the final guideline also had a significantly lower risk of death than those treated with the initial guideline (HR = 0.51, P = 0.046).
Table 3.
The effects of risk factors on transition risks in the illness-death multistate model: Progression from HIV-infected to AIDS and death (with and without progression to AIDS)
|
Variables
|
HIV-Infection → AIDS
|
HIV-Infection → Death
|
AIDS → Death
|
|
HR (95% CI)
|
P
value
|
HR (95% CI)
|
P
value
|
HR (95% CI)
|
P
value
|
| Gender |
|
|
|
|
|
|
| Female |
1.00 |
|
1.00 |
|
1.00 |
|
| Male |
1.02 (0.60, 1.74) |
0.941 |
1.13 (0.52, 2.45) |
0.759 |
1.63 (0.59, 4.52) |
0.413 |
| Age (year) |
|
|
|
|
|
|
| ≤ 30 |
1.00 |
|
1.00 |
|
1.00 |
|
| 31-40 |
1.12 (0.84, 1.50) |
0.446 |
1.17 (0.85, 1.61) |
0.331 |
0.83 (0.52, 1.35) |
0.457 |
| 41-50 |
1.59 (1.06, 2.38) |
0.025 |
2.31 (1.55, 3.45) |
0.001 |
1.29 (0.69, 2.43) |
0.427 |
| > 50 |
3.20 (1.87, 5.46) |
0.001 |
4.23 (2.24, 7.99) |
0.001 |
1.45 (0.45, 3.22) |
0.712 |
| Marital status |
|
|
|
|
|
|
| Other |
1.00 |
|
1.00 |
|
1.00 |
|
| Married |
0.76 (0.56, 1.04) |
0.090 |
0.88 (0.61, 1.28) |
0.515 |
1.41 (0.77, 2.57) |
0.267 |
| Single |
1.10 (0.78, 1.54) |
0.600 |
0.93 (0.64, 1.34) |
0.691 |
1.72 (0.98, 3.00) |
0.059 |
| Education |
|
|
|
|
|
|
| High (high school to academic) |
1.00 |
|
1.00 |
|
1.00 |
|
| Low (illiterate to middle school) |
1.24 (0.89, 1.74) |
0.212 |
1.98 (1.29, 3.06) |
0.002 |
0.86 (0.50, 1.49) |
0.589 |
| Occupational status |
|
|
|
|
|
|
| Unemployed |
1.00 |
|
1.00 |
|
1.00 |
|
| Employed |
0.84 (0.65, 1.10) |
0.209 |
1.10 (0.83, 1.46) |
0.503 |
0.52 (0.33, 0.82) |
0.005 |
| Drug abuse |
|
|
|
|
|
|
| No |
1.00 |
|
1.00 |
|
1.00 |
|
| Yes |
1.00 (0.60, 1.67) |
0.993 |
2.18 (0.97, 4.92) |
0.060 |
1.84 (0.69, 4.98) |
0.224 |
| Imprisonment |
|
|
|
|
|
|
| No |
1.00 |
|
1.00 |
|
1.00 |
|
| Yes |
0.91 (0.64, 1.30) |
0.616 |
1.07 (0.74, 1.55) |
0.704 |
0.57 (0.33, 0.97) |
0.038 |
| Transmission way |
|
|
|
|
|
|
| Unknown |
1.00 |
|
1.00 |
|
1.00 |
|
| Injecting drug user |
1.29 (0.69, 2.40) |
0.428 |
1.41 (0.50, 3.93) |
0.514 |
1.70 (0.48, 6.04) |
0.416 |
| Unprotected sexual |
0.84 (0.46, 1.55) |
0.577 |
3.34 (1.10, 10.21) |
0.034 |
1.33 (0.38, 4.62) |
0.653 |
| Antiretroviral therapy |
|
|
|
|
|
|
| No |
1.00 |
|
1.00 |
|
1.00 |
|
| Yes |
0.43 (0.32, 0.58) |
0.001 |
0.05 (0.03, 0.10) |
0.001 |
0.38 (0.25, 0.58) |
0.001 |
| Tuberculosis infection |
|
|
|
|
|
|
| No |
1.00 |
|
1.00 |
|
1.00 |
|
| Yes |
4.75 (3.32, 6.81) |
0.001 |
0.19 (0.03, 1.37) |
0.099 |
1.90 (1.14, 3.15) |
0.013 |
| Treatment guideline used |
|
|
|
|
|
|
| Initial guideline |
1.00 |
|
1.00 |
|
1.00 |
|
| Intermediate guideline |
1.32 (0.93, 1.86) |
0.116 |
1.15 (0.85, 1.56) |
0.365 |
0.73 (0.44, 1.20) |
0.216 |
| Final guideline |
1.95 (1.31, 2.89) |
0.001 |
0.55 (0.34, 0.88) |
0.014 |
0.51 (0.26, 0.99) |
0.046 |
Note. HIV: Human immunodeficiency virus; AIDS: Acquired immunodeficiency syndrome; HR: Hazard ratio; CI: Confidence interval.
Furthermore, older age at diagnosis significantly intensified the hazard of transition from HIV to AIDS and from HIV to death. The hazard of AIDS progression for HIV-positive individuals aged 41–50 and over 50 was 1.59 (P = 0.025) and 3.20 (P < 0.001) times that of those aged 30 years or less, respectively. Similarly, for patients in these age groups, the hazard of transition from HIV to death was 2.31 (P < 0.001) and 4.23 (P < 0.001) times that of those aged 30 years or less, respectively.
HIV patients with TB were at a higher risk for transition from HIV to AIDS (HR = 4.75, P < 0.001) and from AIDS to death (HR = 1.90, P = 0.013) compared to those without TB infection. Likewise, the risk of direct transition to death was significantly higher among HIV patients with lower levels of education (HR = 1.98, P = 0.002) and those infected through unprotected sexual contact (HR = 3.34, P = 0.034).
In addition, among AIDS patients, unemployed individuals had nearly twice the risk of death compared to employed ones (HR = 0.52, P = 0.005). Similarly, non-prisoners had a higher risk of death than prisoners in this group (HR = 0.57, P = 0.028).
Discussion
The present study described the progression of HIV disease using an illness-death model that encompasses the transitions from HIV to AIDS, from AIDS to death, and from HIV to death, and investigated the effect of several risk factors on the occurrence of these transitions. Of the risk factors examined in this study, ART and the applied treatment guideline significantly affected the hazard of all three transitions. Age at diagnosis and TB influenced the hazard of transition from HIV to AIDS. Education, mode of transmission, and age at diagnosis impacted the hazard of transition from HIV to death. Finally, occupational status and imprisonment, and TB affected the hazard of transition from AIDS to death.
The findings of this study confirm that receiving ART had a key role in reducing the risk of HIV progression to AIDS, as well as the risk of death, both following AIDS and without its development. There were 57%, 95%, and 62% reductions in progression to AIDS, death without AIDS, and death after AIDS, respectively, compared to those who did not receive treatment. These findings highlight the strong protective effect of ART, consistent with the results of previous studies.10,19,22,23,32,33 Hence, early diagnosis and timely treatment should be prioritized to improve patient outcome.
It was also found that patients treated with the final guideline had twice the risk of progressing to AIDS compared to those treated with the initial guideline, while their risk of death with or without AIDS was reduced by half. The higher AIDS progression for patients may be due to better screening and detection of HIV, even in late stages, along with delayed diagnosis, treatment initiation, or poor adherence to therapy when this treatment guideline was applied. However, improved care and easier access helped reduce the risk of death.5,34-36
Moreover, the results indicated that patients co-infected with TB had a substantially higher risk of developing AIDS and dying from it, which is consistent with results of other studies.10,11,16,23,25 On the other hand, TB co-infection did not significantly affect the hazard of transition from HIV to death, which aligns with the findings of some studies while contradicting those of others.9,10,13,19,32
Our findings revealed that patients with older age at the time of diagnosis had a higher risk for both HIV-to-AIDS and HIV-to-death transitions, which corroborates the results of many studies.10,12,22,25,37-39 They may be attributed to the association of older age with factors such as lower CD4 counts, more advanced disease stages, and delayed diagnosis.5,40,41
In the present study, HIV patients with a lower level of education were more likely to experience direct death, which conforms to the findings of other studies.13,42 In addition, individuals infected through sexual transmission were at a higher risk of death without developing AIDS compared to those with unknown transmission. This difference may be due to individuals infected sexually being more likely to acquire co-infections, such as human papillomavirus, syphilis, candidiasis, and herpes, which weaken the immune system and increase the risk of death.12,43 However, this finding should be interpreted with caution, as individuals may have been exposed to multiple routes of transmission, and it is often impossible to accurately determine the primary route of transmission from the limited data recorded.
In contrast to Cook et al,44 who reported no significant effect, the results of this study are consistent with those of Gheibi et al, demonstrating that employment was significantly associated with a reduced hazard of AIDS-related mortality.38 The findings also revealed a significant protective association between the risk of death and imprisonment among patients with AIDS, contrasting with the findings of Amiri et al45 Similar to previous studies, the reduced risk of death among prisoners in this study may be due to access to free and supervised ART, improved adherence, and reduced exposure to high-risk behaviors.13,46
In this study, the cumulative risk of transition from AIDS to death was higher than that of transition from HIV to death, indicating that AIDS-related mortality occurred with greater intensity over time. However, our results also confirmed that deaths were more frequent overall in patients without AIDS progression. Before the implementation of the final guideline, mortality in this group was more than twice as high as in patients with AIDS; thereafter, the numbers were almost the same. This not only highlights the importance of timely ART initiation in HIV-positive patients without progression to AIDS but also emphasizes the need to focus more on non-AIDS-related causes of death in this population to effectively reduce overall mortality. Although we did not have data on the specific causes of death, the occurrence of mortality among patients without AIDS progression emphasizes the need for further investigation into non-AIDS-related factors.
It should be noted that Hamidi et al applied a multistate model to analyze the HIV data from Hamadan. Their study was limited to data up to 2011 and included individuals of all age groups.10 In contrast, our study focused on adult patients and considered a longer follow-up period up to 2023, which allowed for an assessment of treatment guidelines and their impact on disease progression and mortality.
This study had two limitations, as it used retrospective data collected in a health center. First, two important prognostic markers, baseline CD4 cell count and HIV viral load, were largely unavailable for patients diagnosed before 2011, because viral load was not measured at baseline according to the national guidelines at that time, and baseline CD4 count was not routinely assessed for most individuals referred during the early years of the outbreak. Second, some important factors, including late diagnosis, body mass index, treatment adherence, co-infection with hepatitis B or C, underlying diseases, and other opportunistic infections, were either not recorded or were incompletely documented, which could have affected HIV disease progression.
It is worth noting that variables for the final multistate model were selected based on univariate multistate models. However, for future work, it is suggested to apply variable selection procedures for multistate data, such as the method proposed by Alafchi et al, to identify the most influential predictors.47
Highlights
-
In this study, 329 patients died, of whom 109 (33%) died after progressing to acquired immunodeficiency syndrome (AIDS) and 220 (67%) died without AIDS progression. In other words, deaths without the progression of AIDS occurred more frequently.
-
The cumulative hazard of transition from AIDS to death was higher than that from HIV to death.
-
Receiving antiretroviral therapy (ART) significantly decreased the hazard of transition from HIV to AIDS, from human immunodeficiency virus (HIV) to death, and from AIDS to death.
-
Patients aged 40 and over, with lower levels of education and unprotected sexual transmission, had a higher risk of transition from HIV to death.
Conclusion
In this study, the effect of prognostic factors on progression from HIV to AIDS and death, with or without developing AIDS, was assessed using a multistate model. The findings revealed that patients who received ART and were treated with the final guideline had a reduced risk of death, either with or without AIDS progression. TB intensified the risk of both AIDS progression and AIDS-related death. In addition, the cumulative hazard of AIDS-related death increased markedly over time, and the number of deaths directly attributable to HIV was high. These findings demonstrated that strict implementation of the ‘treat all HIV-positive patients’ strategy could be useful in reducing progression to AIDS and mortality. Furthermore, they highlighted the importance of implementation strategies for early diagnosis, timely treatment, and adherence to treatment, as well as screening and TB treatment, especially at younger ages, for both health providers and policymakers.
Acknowledgements
This work was a part of a PhD thesis in biostatistics submitted by Roghayyeh Hassanzadeh to Hamadan University of Medical Sciences, Iran. We would like to thank the Vice-Chancellor for Research and Technology of Hamadan University of Medical Sciences, Iran.
Competing Interests
The authors declare that they have no competing and conflict of interests.
Ethical Approval
This study was approved by the Research Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1400.910), and the study complied with the relevant guidelines and regulations. Written informed consent was obtained from all participants; in the case of illiterate participants, it was obtained from their legal representatives with confidentiality regarding the patients’ names and surnames.
Funding
The study was supported by the Vice-Chancellor for Research and Technology, Hamadan University of Medical Sciences (Grant No. 1400120310201).
References
- World Health Organization (WHO). HIV and AIDS. WHO; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids. Accessed 2025.
- World Health Organization (WHO). Why the HIV Epidemic is Not Over. WHO; 2023. Available from: https://www.who.int/news-room/spotlight/why-the-hiv-epidemic-is-not-over. Accessed 2025.
- UNAIDS. Islamic Republic of Iran. UNAIDS; 2023. Available from: https://www.unaids.org/en/regionscountries/countries/islamicrepublicofiran. Accessed 2025.
- Hileman CO, Funderburg NT. Inflammation, immune activation, and antiretroviral therapy in HIV. Curr HIV/AIDS Rep 2017; 14(3):93-100. doi: 10.1007/s11904-017-0356-x [Crossref] [ Google Scholar]
- Mohammadi Y, Mirzaei M, Shirmohammadi-Khorram N, Farhadian M. Identifying risk factors for late HIV diagnosis and survival analysis of people living with HIV/AIDS in Iran (1987-2016). BMC Infect Dis 2021; 21(1):390. doi: 10.1186/s12879-021-06100-z [Crossref] [ Google Scholar]
- Poorolajal J, Hooshmand E, Mahjub H, Esmailnasab N, Jenabi E. Survival rate of AIDS disease and mortality in HIV-infected patients: a meta-analysis. Public Health 2016; 139:3-12. doi: 10.1016/j.puhe.2016.05.004 [Crossref] [ Google Scholar]
- Fuge TG, Tsourtos G, Miller ER. Risk factors for late linkage to care and delayed antiretroviral therapy initiation among adults with HIV in sub-Saharan Africa: a systematic review and meta-analyses. Int J Infect Dis 2022; 122:885-904. doi: 10.1016/j.ijid.2022.07.037 [Crossref] [ Google Scholar]
- Granich R, Gupta S, Hersh B, Williams B, Montaner J, Young B. Trends in AIDS deaths, new infections and ART coverage in the top 30 countries with the highest AIDS mortality burden; 1990-2013. PLoS One 2015; 10(7):e0131353. doi: 10.1371/journal.pone.0131353 [Crossref] [ Google Scholar]
- Akbari M, Fararouei M, Haghdoost AA, Gouya MM, Afsar Kazerooni P. Survival and associated factors among people living with HIV/AIDS: A 30-year national survey in Iran. J Res Med Sci 2019; 24:5. doi: 10.4103/jrms.JRMS_630_18 [Crossref] [ Google Scholar]
- Hamidi O, Tapak L, Poorolajal J, Amini P. Identifying risk factors for progression to AIDS and mortality post-HIV infection using illness-death multistate model. Clin Epidemiol Glob Health 2017; 5(4):163-8. doi: 10.1016/j.cegh.2017.08.003 [Crossref] [ Google Scholar]
- Tapak L, Kosorok MR, Sadeghifar M, Hamidi O. Multistate recursively imputed survival trees for time-to-event data analysis: an application to AIDS and mortality post-HIV infection data. BMC Med Res Methodol 2018; 18(1):129. doi: 10.1186/s12874-018-0596-5 [Crossref] [ Google Scholar]
- Jia XC, Xia ZH, Shi N, Wang YP, Luo ZX, Yang YL. The factors associated with natural disease progression from HIV to AIDS in the absence of ART, a propensity score matching analysis. Epidemiol Infect 2020; 148:e57. doi: 10.1017/s0950268820000540 [Crossref] [ Google Scholar]
- Najafi Ghobadi KN, Roshanaei G, Poorolajal J, Shakiba E, Khassi K, Mahjub H. The estimation of long- and short-term survival time and associated factors of HIV patients using mixture cure rate models. BMC Med Res Methodol 2023; 23(1):123. doi: 10.1186/s12874-023-01949-x [Crossref] [ Google Scholar]
- Haynes BF, Pantaleo G, Fauci AS. Toward an understanding of the correlates of protective immunity to HIV infection. Science 1996; 271(5247):324-8. doi: 10.1126/science.271.5247.324 [Crossref] [ Google Scholar]
- Dessie ZG, Zewotir T, Mwambi H, North D. Modelling of viral load dynamics and CD4 cell count progression in an antiretroviral naive cohort: using a joint linear mixed and multistate Markov model. BMC Infect Dis 2020; 20(1):246. doi: 10.1186/s12879-020-04972-1 [Crossref] [ Google Scholar]
- Mirzaei M, Poorolajal J, Khazaei S, Saatchi M. Survival rate of AIDS disease and mortality in HIV-infected patients in Hamadan, Iran: a registry-based retrospective cohort study (1997-2011). Int J STD AIDS 2013; 24(11):859-66. doi: 10.1177/0956462413486457 [Crossref] [ Google Scholar]
- Mirzaei H, Eybpoosh S, Mehrabi F, Shojaei MR, Mirzazadeh A, Khezri M. Prevalence of acquired and transmitted HIV drug resistance in Iran: a systematic review and meta-analysis. BMC Infect Dis 2024; 24(1):29. doi: 10.1186/s12879-023-08916-3 [Crossref] [ Google Scholar]
- McManus H, O’Connor CC, Boyd M, Broom J, Russell D, Watson K. Long-term survival in HIV positive patients with up to 15 Years of antiretroviral therapy. PLoS One 2012; 7(11):e48839. doi: 10.1371/journal.pone.0048839 [Crossref] [ Google Scholar]
- Najafi Ghobadi K, Mahjub H, Poorolajal J, Shakiba E, Khassi K, Roshanaei G. Joint modeling of longitudinal outcome and competing risks: application to HIV/AIDS data. J Res Health Sci 2023; 23(1):e00571. doi: 10.34172/jrhs.2023.106 [Crossref] [ Google Scholar]
- Vivithanaporn P, Kongratanapasert T, Suriyapakorn B, Songkunlertchai P, Mongkonariyawong P, Limpikirati PK. Potential drug-drug interactions of antiretrovirals and antimicrobials detected by three databases. Sci Rep 2021; 11(1):6089. doi: 10.1038/s41598-021-85586-8 [Crossref] [ Google Scholar]
- Bojdy A, Arian M, Najaf Najafi M, Mottaghi M. Adherence to antiretroviral therapy and its determinants in HIV patients in Mashhad, Iran, 2018: a prospective study. Rev Clin Med 2020; 7(4):157-62. doi: 10.22038/rcm.2020.52601.1339 [Crossref] [ Google Scholar]
- Alafchi B, Tapak L, Mahjub H, Talebi Ghane E, Roshanaei G. Joint modelling of longitudinal ordinal and multi-state data. Stat Methods Med Res 2024; 33(11-12):1939-51. doi: 10.1177/09622802241281013 [Crossref] [ Google Scholar]
- Mirzaei M, Farhadian M, Poorolajal J, Afsar Kazerooni P, Tayeri K, Mohammadi Y. Survival rate and the determinants of progression from HIV to AIDS and from AIDS to the death in Iran: 1987 to 2016. Asian Pac J Trop Med 2019; 12(2):72-8. doi: 10.4103/1995-7645.250840 [Crossref] [ Google Scholar]
- Jiang H, Xie N, Cao B, Tan L, Fan Y, Zhang F. Determinants of progression to AIDS and death following HIV diagnosis: a retrospective cohort study in Wuhan, China. PLoS One 2013; 8(12):e83078. doi: 10.1371/journal.pone.0083078 [Crossref] [ Google Scholar]
- Poorolajal J, Molaeipoor L, Mohraz M, Mahjub H, Taghizadeh Ardekani M, Mirzapour P. Predictors of progression to AIDS and mortality post-HIV infection: a long-term retrospective cohort study. AIDS Care 2015; 27(10):1205-12. doi: 10.1080/09540121.2015.1045405 [Crossref] [ Google Scholar]
- Andersen PK, Keiding N. Multi-state models for event history analysis. Stat Methods Med Res 2002; 11(2):91-115. doi: 10.1191/0962280202SM276ra [Crossref] [ Google Scholar]
- Andersen PK, Pohar Perme M. Inference for outcome probabilities in multi-state models. Lifetime Data Anal 2008; 14(4):405-31. doi: 10.1007/s10985-008-9097-x [Crossref] [ Google Scholar]
- de Wreede LC, Fiocco M, Putter H. The mstate package for estimation and prediction in non- and semi-parametric multi-state and competing risks models. Comput Methods Programs Biomed 2010; 99(3):261-74. doi: 10.1016/j.cmpb.2010.01.001 [Crossref] [ Google Scholar]
- Meira-Machado L, de Uña-Alvarez J, Cadarso-Suárez C, Andersen PK. Multi-state models for the analysis of time-to-event data. Stat Methods Med Res 2009; 18(2):195-222. doi: 10.1177/0962280208092301 [Crossref] [ Google Scholar]
- World Health Organization (WHO). WHO Case Definitions of HIV For Surveillance and Revised Clinical Staging and Immunological Classification of HIV-Related Disease in Adults and Children. Geneva: WHO; 2007.
- Radfar S, Tayeri K, Namdari Tabar H. Practical Guidelines on How to Provide Consulting Services in Behavioral Disorders Centers. Tehran: Ministry of Health and Medical Education; 2009.
- Seyoum D, Degryse JM, Kifle YG, Taye A, Tadesse M, Birlie B. Risk factors for mortality among adult HIV/AIDS patients following antiretroviral therapy in Southwestern Ethiopia: an assessment through survival models. Int J Environ Res Public Health 2017; 14(3):296. doi: 10.3390/ijerph14030296 [Crossref] [ Google Scholar]
- Teeraananchai S, Kerr SJ, Amin J, Ruxrungtham K, Law MG. Life expectancy of HIV-positive people after starting combination antiretroviral therapy: a meta-analysis. HIV Med 2017; 18(4):256-66. doi: 10.1111/hiv.12421 [Crossref] [ Google Scholar]
- Sharafi M, Mirahmadizadeh A, Hassanzadeh J, Seif M, Heiran A. Factors associated with late initiation of antiretroviral therapy in Iran’s HIV/AIDS surveillance data. Sci Rep 2024; 14(1):199. doi: 10.1038/s41598-023-50713-0 [Crossref] [ Google Scholar]
- Siraj M, Gedamu S, Tegegne B. Predictors of survival time among HIV-infected adults after initiating anti-retroviral therapy in Kombolcha town: a 5-year retrospective cohort study. HIV AIDS (Auckl) 2022; 14:181-94. doi: 10.2147/hiv.S359495 [Crossref] [ Google Scholar]
- Chegene Lorestani R, Kazemisafa N, Rostamian M, Akya A, Rezaeian S, Bashiri H. Survival-related factors in HIV/AIDS patients: a retrospective cohort study from 2011 to 2019 in Kermanshah, Iran. Curr HIV Res 2022; 20(5):419-27. doi: 10.2174/1570162x20666220617141619 [Crossref] [ Google Scholar]
- Matsena Zingoni Z, Chirwa TF, Todd J, Musenge E. HIV disease progression among antiretroviral therapy patients in Zimbabwe: a multistate Markov model. Front Public Health 2019; 7:326. doi: 10.3389/fpubh.2019.00326 [Crossref] [ Google Scholar]
- Gheibi Z, Shayan Z, Joulaei H, Fararouei M, Beheshti S, Shokoohi M. Determinants of AIDS and non-AIDS related mortality among people living with HIV in Shiraz, southern Iran: a 20-year retrospective follow-up study. BMC Infect Dis 2019; 19(1):1094. doi: 10.1186/s12879-019-4676-x [Crossref] [ Google Scholar]
- Hamidi O, Poorolajal J, Tapak L. Identifying predictors of progression to AIDS and mortality post-HIV infection using parametric multistate model. Epidemiol Biostat Public Health 2017; 14(2):e12438-9. doi: 10.2427/12438 [Crossref] [ Google Scholar]
- Montarroyos UR, Miranda-Filho DB, César CC, Souza WV, Lacerda HR, de Fátima Pessoa Militão Albuquerque M. Factors related to changes in CD4 + T-cell counts over time in patients living with HIV/AIDS: a multilevel analysis. PLoS One 2014; 9(2):e84276. doi: 10.1371/journal.pone.0084276 [Crossref] [ Google Scholar]
- Kyaw AT, Sawangdee Y, Hunchangsith P, Pattaravanich U. Survival rate and socio-demographic determinants of mortality in adult HIV/AIDS patients on anti-retrovial therapy (ART) in Myanmar: a registry based retrospective cohort study 2005-2015. J Health Res 2017; 31(4):323-31. doi: 10.14456/jhr.2017.40 [Crossref] [ Google Scholar]
- Rubaihayo J, Tumwesigye NM, Konde-Lule J, Makumbi F, Nakku EJ, Wamani H. Trends and predictors of mortality among HIV positive patients in the era of highly active antiretroviral therapy in Uganda. Infect Dis Rep 2015; 7(3):5967. doi: 10.4081/idr.2015.5967 [Crossref] [ Google Scholar]
- Mukanyangezi MF, Manzi O, Tobin G, Rulisa S, Bienvenu E, Giglio D. Sexual risk behaviour in a cohort of HIV-negative and HIV-positive Rwandan women. Epidemiol Infect 2018; 147:e54. doi: 10.1017/s0950268818003023 [Crossref] [ Google Scholar]
- Cook JA, Grey D, Burke J, Cohen MH, Gurtman AC, Richardson JL. Depressive symptoms and AIDS-related mortality among a multisite cohort of HIV-positive women. Am J Public Health 2004; 94(7):1133-40. doi: 10.2105/ajph.94.7.1133 [Crossref] [ Google Scholar]
- Amiri F, Roshanaei G, Olfati Far M, Najafi R, Poorolajal J. Survival analysis of the human immunodeficiency virus in Iranian patients: a multistate model. J Arak Uni Med Sci 2021; 24(2):180-95. doi: 10.32598/jams.24.2.5530.2.[Persian] [Crossref] [ Google Scholar]
- Dolan K, Wirtz AL, Moazen B, Ndeffo-Mbah M, Galvani A, Kinner SA. Global burden of HIV, viral hepatitis, and tuberculosis in prisoners and detainees. Lancet 2016; 388(10049):1089-102. doi: 10.1016/s0140-6736(16)30466-4 [Crossref] [ Google Scholar]
- Alafchi B, Tapak L, Doosti H, Chesneau C, Roshanaei G. A two-step algorithm to estimate variable importance for multi-state data: an application to COVID-19. Comput Model Eng Sci 2023; 135(3):2047-64. doi: 10.32604/cmes.2022.022647 [Crossref] [ Google Scholar]