J Res Health Sci. 23(4):e00596.
doi: 10.34172/jrhs.2023.131
Original Article
The Effect of Community-Based Intervention on Dengue Awareness and Prevention Among Poor Urban Communities in Delhi, India
Abhishek Lachyan 1  , Rafdzah Ahmad Zaki 1, * , Bratati Banerjee 2, Nasrin Aghamohammadi 1, 3
, Rafdzah Ahmad Zaki 1, * , Bratati Banerjee 2, Nasrin Aghamohammadi 1, 3
Author information:
1Center for Epidemiology and Evidence-Based Practice, Department of Social and Preventive Medicine, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysia
2Department of Community Medicine, Maulana Azad Medical College, New Delhi, India
3School Design and the Built Environment, Curtin University Sustainability Policy Institute, Kent St, Bentley, 6102, Western Australia
Abstract
Background: This study aimed to assess the efficacy of a dengue intervention program in economically deprived urban regions of India, with a particular emphasis on housing conditions and community involvement. Given the global significance of dengue fever as a vector-borne disease, successful vector management requires effective community engagement.
Study Design: A quasi-experimental study.
Methods: This study was conducted with 314 participants from Delhi’s Sanjay Colony, divided into control and intervention groups. The study spanned 14 months (August 2020 to September 2021). The intervention program comprised two educational sessions held one month apart, covering dengue awareness, health self-care, and environmental maintenance. Data were collected at baseline, after each intervention session, and during a final follow-up assessment three months later.
Results: The primary outcome, the house index (HI), revealed statistically significant differences (P<0.001) favoring the intervention group. The total score (TS) for mosquito-borne disease, TS of knowledge, TS of attitude, and TS of practices all exhibited significant improvements in the intervention group. Participants showed an enhanced understanding of dengue causes, symptoms, and mosquito behavior related to breeding and biting. The HI in the intervention group decreased significantly from 21.65% to 4.45% (P<0.05).
Conclusion: This study, grounded in the health belief model (HBM), demonstrated the effectiveness of the intervention program in reducing HI and improving knowledge and preventive practices regarding dengue fever in impoverished urban neighborhoods of Delhi. The intervention program may be beneficial in such a poor urban community.
Keywords: Community-based intervention, Dengue, Housing, Prevention
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Lachyan A, Zaki RA, Banerjee B, Aghamohammadi N. The effect of community-based intervention on dengue awareness and prevention among poor urban communities in Delhi, India. J Res Health Sci. 2023; 23(4):e00596s. doi:10.34172/ jrhs.2023.131
Background
Dengue fever, a rapidly spreading virus transmitted by mosquitoes, stands as a formidable global public health challenge.1 The magnitude of this problem is underscored by the staggering surge in cases by a factor of 30 over the past five decades. According to the World Health Organization, dengue has witnessed a worldwide incidence rate increase of approximately 30% annually. The mortality rate, though comparatively lower, is significant, with approximately 20 000 deaths reported globally each year.2,3 Additionally, the disability caused by dengue, including the long-term health impacts on survivors, adds another layer of concern, affecting approximately 500 000 individuals annually.4
In India, where the climate is conducive to dengue transmission, the National Vector Borne Diseases Control Programme (NVBDCP) has been actively engaged in prevention and management efforts.5 However, the incidence rate of dengue in the country remains a critical concern, particularly after the monsoon season, when Aedes mosquitoes, the primary vectors, thrive in artificial water containers near homes, factories, and construction sites.6
Effective dengue control demands a comprehensive strategy, encompassing vector surveillance, integrated mosquito management, environmental upkeep, legislation, and crucially, community involvement.7 Health education emerges as a linchpin in this strategy, and the NVBDCP employs diverse communication channels to educate populations in endemic regions.8
The health belief model (HBM), rooted in social psychology theory, informs the preventive strategies of this study. According to the HBM, individuals are more likely to adopt disease prevention practices when they perceive the benefits, encounter fewer barriers, receive cues to prompt action, face modifying factors, and possess the motivation to stay healthy.9-12 Recognizing the pivotal role of community involvement in dengue control, this study focuses on raising awareness, enhancing the understanding of disease risks, emphasizing prevention benefits, and removing obstacles to preventive actions.13-18 The goal is to assess how a community-based intervention can contribute to increased awareness and reduced dengue incidence, particularly in the impoverished urban areas of Delhi.
Methods
The purpose of this study is to examine the effectiveness of the intervention program for dengue fever prevention among poor urban communities in Delhi, India, based on the theory of HBM.
Study Design and Duration
As mentioned earlier, this quasi-experimental research aimed to evaluate the effectiveness of dengue fever prevention strategies in poor urban communities. With a control group, this study employed a quasi-experimental approach. Following the session, this group completed a post-intervention evaluation. A control group receives pre- and post-tests and no intervention simultaneously as the other groups. These research techniques are often used to investigate educational programs’ effectiveness.
Studies to evaluate interventions without the use of randomization are called quasi-experiments. Similar to randomized trials, quasi-experiments seek to show that an intervention causes an effect. Preintervention and postintervention assessments and groups that are not randomly selected can all be utilized in quasi-experimental studies. This study could not adopt a randomized control trial design because participant randomization took a lot of work. Randomizing the intervention for each participant is frequently tricky. The other reason for not adopting the mentioned design was the difficulty of location-based randomization (e.g., colony). Similar difficulties arise when attempting to randomize interventions to specific places, as well as dengue therapies to specific sites. Using the dengue knowledge, attitude, and practice (KAP) example, applying the system in some hospitals or areas might be challenging. Let us declare that the dengue KAP includes a learning component. If that happened, it may appear that the intervention was unsuccessful because people would likely apply what they had learned to a colony that was not a member of the KAP. Participants were randomly divided into a control group continuing their routine practices and an experimental group undergoing a three-month intervention (Figure 1). Data were collected before (baseline), immediately after, and during a final follow-up (3-month intervention and 1-month final follow-up). The study was conducted between August 2020 and September 2021 (Figure 2).
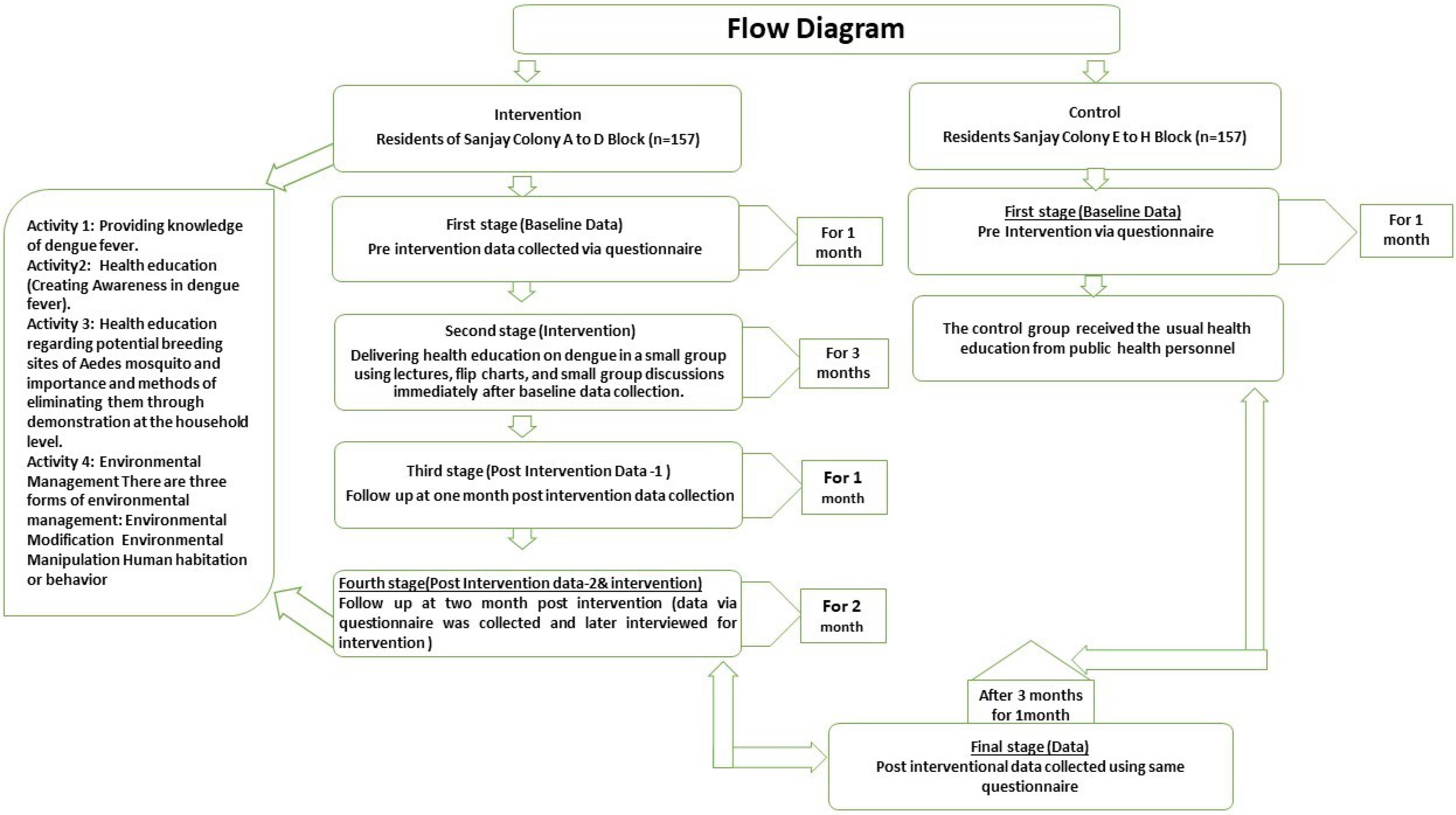
Figure 1.
The Study Flow Chart
.
The Study Flow Chart
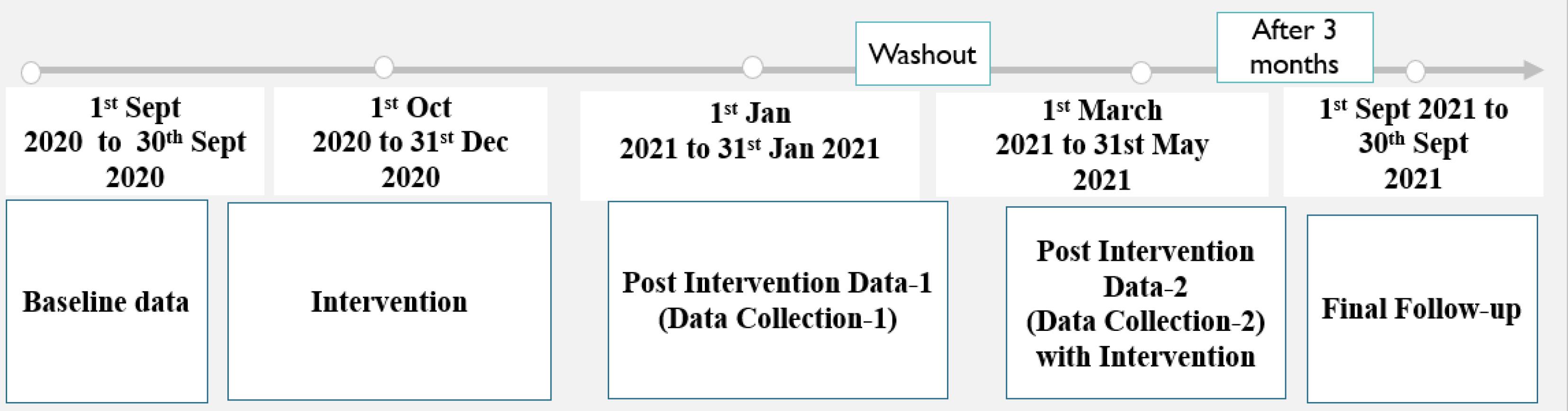
Figure 2.
Timeline of Research
.
Timeline of Research
Participant Selection
Residents aged 18 years were included, and one member was randomly selected in households with multiple eligible members. The inclusion criteria also encompassed a residency of over a year in the study area, the ability for effective communication, and the willingness to participate. On the other hand, the exclusion criteria were applied to individuals with serious illnesses and conditions affecting participation.
Sampling Method
The study utilized systematic random sampling to select households, applying a formula to calculate the sampling interval (k) and ensuring a sample size of 157 for each group. The sample size needed for this study was 157 for each group.
Questionnaire Structure
The questionnaire structure employed in the study followed a pre-tested, closed-ended format. To ensure the validity and reliability of the questionnaire, content validity, including expert validation of the questionnaire and measurement instrument, was assessed through testing. Additionally, the reliability of the questionnaire was confirmed using Cronbach’s alpha coefficient.
Interventions Implemented
In the study, participants in the control group received no interventions, serving as a comparison against those in the intervention group. Participants in the intervention group were enrolled in a program guided by the HBM theory. The interventions implemented in this group were diverse, incorporating a range of strategies aimed at bolstering community awareness and fostering engagement in dengue prevention efforts. Further details about these interventions are provided in Table 1 and Figure 1.
Table 1.
The details of interventions implemented in the study
|
Activity
|
Description
|
| Public awareness on dengue fever |
Daily local broadcasts designed based on the health belief model components: Increasing susceptibility, highlighting severity, emphasizing benefits, and reducing barriers |
| Health education (Creating dengue fever awareness) |
- Dissemination of health information through lectures, flip charts, and small group discussions
- Distribution of pamphlets and posters on dengue prevention techniques and guidelines from the Dengue Control Division
- Information on using Temephos (Abate sand) and insect repellent to eliminate larvae
- Distribution of pamphlets with information about dengue disease, including warning signs and symptoms |
| Household-level health education on Aedes mosquito breeding |
Face-to-face training sessions with families, covering Aedes mosquitoes’ breeding sites and emphasizing prompt cleaning and container covering
Community-level education included street plays to raise awareness
The standardized larval survey format was conducted in 157 homes, calculating house index, container index, and Breteau index |
| Environmental management |
Collaboration with community leaders and Delhi’s Municipal Corporations. Environmental modification, manipulation, and human habitation or behaviour approaches implemented to prevent dengue
Municipality incorporated recommendations post-study, resulting in infrastructure improvements and enhanced essential services |
Data Collection Instrument
The questionnaire was structured into sections on socio-demographics, knowledge, attitude, and preventive practices. The questions were designed to assess participants’ understanding, attitudes, and behaviors related to dengue fever.
Section I: Socio-demographic profiles: This section aimed to gather essential socio-demographic information about the participants, providing a foundation for understanding the context in which their KAPs regarding dengue fever were situated.
Section II: Knowledge: Comprising 21 questions, this section focused on assessing participants’ understanding of the risk factors associated with dengue fever. Each question was scored with 1 for ‘Yes’ and 0 for ‘No’, and the overall knowledge was evaluated using mean scores, offering a quantitative measure of participants’ comprehension of dengue fever.
Section III: Attitudes: This section, consisting of 6 questions, delved into participants’ attitudes toward dengue fever as a disease. Responses were measured on a Likert-type scale, ranging from 5 (Strongly agree) to 1 (Not sure). Mean scores were again used to gauge the overall attitude of the study participants, providing insight into their conscious awareness of dengue fever risk factors.
Section IV: Preventive Practices: With 19 questions, this section focused on participants’ self-reported practices to prevent dengue fever. The responses were scored as 1 for ‘Yes’ and 0 for ‘No’, reflecting the implementation of preventive measures. This section sought to capture the practical aspects of participants’ behavior related to dengue fever prevention.
The study applied a systematic approach by incorporating a combination of closed-ended questions, Likert-type scale responses, and scoring mechanisms to quantitatively evaluate the KAP of the target population regarding dengue fever. The use of mean scores facilitated a more nuanced understanding of the participants’ overall awareness, attitudes, and behavioral practices in the context of dengue fever, contributing valuable insights into public health interventions and education campaigns.
To ensure dependability, 30 individuals possessing similar characteristics as the study samples were employed to evaluate the questionnaire’s reliability. The internal consistency and reliability of the questionnaire were confirmed through the examination of Cronbach’s alpha (α) coefficient, which yielded excellent internal consistency values of at least 0.80 across all scales. The clarity, informativeness, and overall coherence of the questions underwent assessment. All questions were formulated as open-ended queries, and the responses were meticulously reviewed and grouped based on similarities. Data entry and descriptive analysis were conducted using SPSS software, version 25.
Intervention Program Evaluation
To assess the effectiveness of the intervention program, data were collected before, immediately after, and during a final follow-up. Changes in the house index (HI) were a primary outcome measure, demonstrating a significant decrease in the intervention group.
In-Depth Analysis
The study aimed to facilitate in-depth analysis by employing a quasi-experimental design. This design allowed for a comprehensive evaluation of the intervention’s impact in a real-world setting, considering the complexities of poor urban communities in Delhi. The quasi-experimental approach was chosen due to the practical challenges of participant randomization and location-based randomization. These challenges, including the intricate process of randomizing interventions to specific places, were addressed by adopting a quasi-experimental design, ensuring a pragmatic yet rigorous evaluation of dengue prevention strategies.
Statistical Analysis
The information was gathered on a Microsoft Redmond Campus MS Office Excel Sheet (version 2019), Redmond, Washington, USA. The data were examined using SPSS (version 25.0, IBM), a statistical package for the social sciences. A coding system that has been checked for entry errors is provided by statistical analysis to reveal all the data entered into the computer. Descriptive statistics, such as frequencies and percentages, as well as means and standard deviations (SD), have been shown for categorical and numerical data, respectively. The chi-square test compared the frequencies of various variable categories within the group. A t-test was used to compare the two groups, and a repeated measures ANOVA (for more than two observations) and a post hoc test were employed for comparison within the same group. With an error of between 5% and 20% for all statistical tests, P > 0.05 was deemed statistically significant, giving the study power of 80%. The following notations apply to all tables:
# = Non-significant difference (P> 0.05), ** = Statistically very significant difference (P< 0.01), and * = Statistically significant difference (P< 0.05).
The difference in the number of HIs between the two groups was analyzed using the χ2 test.
Results
Table 2 presents a comprehensive breakdown of the distribution and comparison of demographic factors between the control and intervention groups. The factors influencing the desired outcomes do not differ between the control and intervention groups; the baseline sociodemographic characteristics of both groups were the same (Table 1). Apart from occupation, where it was observed that the majority of participants were employed in various industrial settings, there were no significant variations in the overall characteristics of the intervention and control groups.
Table 2.
Comparison of thesociodemographic differences between the intervention and control groups
|
Variables
|
Control (n=157)
|
Intervention (n=157)
|
χ2
|
P value
|
|
Number
|
Percent
|
Number
|
Percent
|
| Gender |
|
|
|
|
|
|
| Male |
78 |
49.69 |
77 |
49.04 |
0.000 |
1.000 |
| Female |
79 |
50.31 |
80 |
50.96 |
| Age |
|
|
|
|
|
|
| 18-27 |
40 |
25.47 |
38 |
24.20 |
6.684 |
0.154 |
| 28-37 |
44 |
28.02 |
37 |
23.56 |
| 38-47 |
46 |
29.29 |
40 |
25.47 |
| 48- 57 |
21 |
13.37 |
25 |
15.95 |
| 58 and above |
6 |
03.85 |
17 |
10.82 |
| Education |
|
|
|
|
|
|
| Illiterate |
14 |
08.91 |
4 |
02.56 |
10.482 |
0.063 |
| Primary |
72 |
45.88 |
73 |
46.49 |
| Secondary |
41 |
26.11 |
58 |
36.94 |
| Collegiate |
30 |
19.10 |
22 |
14.01 |
| Occupation |
|
|
|
|
|
|
| Unemployed |
18 |
11.46 |
7 |
04.45 |
54.024 |
0.001 |
| Housewife |
45 |
28.66 |
23 |
14.64 |
| Student |
3 |
01.94 |
6 |
03.82 |
| Aged population |
6 |
03.82 |
10 |
06.36 |
| Private job |
46 |
29.29 |
25 |
15.96 |
| Government job |
8 |
05.09 |
00 |
00.00 |
| Self-employed |
31 |
19.74 |
86 |
54.77 |
| Types of family |
|
|
|
|
|
|
| Nuclear family |
131 |
83.43 |
135 |
85.99 |
0.393 |
0.530 |
| Joint family |
26 |
16.57 |
22 |
14.01 |
| Religion |
|
|
|
|
|
|
| Hindu |
153 |
97.45 |
153 |
97.45 |
0.140 |
0.709 |
| Muslim |
4 |
02.54 |
4 |
02.54 |
| Marital status |
|
|
|
|
|
|
| Married |
150 |
95.46 |
145 |
92.35 |
1.401 |
0.237 |
| Unmarried |
7 |
04.45 |
12 |
07.65 |
| Income (Rs) |
|
|
|
|
|
|
| ≥ 7533 |
157 |
100 |
151 |
96.17 |
6.117 |
0.047 |
| 3766-7532 |
0 |
00.00 |
5 |
03.18 |
| 1130-2259 |
0 |
00.00 |
1 |
0.65 |
Table 3 provides an initial comparison of total scores (TS) between the intervention and control groups, emphasizing factors such as mosquito-induced illnesses, knowledge, attitude, and behaviors. The initial “t” value for the variable “Disease caused by mosquitoes” was -0.830. However, upon closer examination, no statistically significant difference between the groups was observed at the beginning (P-value > 0.05).
Table 3.
Intergroups comparison of scores at baseline total score (n = 157)
|
Variables
|
Mean
|
SD
|
SE
|
P value
|
| Total score for disease caused by mosquitoes |
| Control |
1.92 |
0.967 |
0.077 |
0.407 |
| Intervention |
2.01 |
0.937 |
0.075 |
| Total score knowledge |
|
|
|
|
| Control |
10.48 |
3.407 |
0.380 |
0.788 |
| Intervention |
10.64 |
2.871 |
0.453 |
| Total score attitude |
|
|
|
|
| Control |
20.71 |
4.497 |
0.359 |
0.777 |
| Intervention |
20.83 |
3.398 |
0.271 |
| Total score practices |
|
|
|
|
| Control |
4.37 |
1.882 |
0.150 |
0.077 |
| Intervention |
3.99 |
1.869 |
0.149 |
Note. SD: Standard deviation; SE: Standard error.
Based on the data (Table 4) obtained in the final follow-up, the “t” value for the variable “Disease caused by mosquitoes” was 30.316 when comparing the intervention and control groups. Subsequent analysis indicated a statistically significant difference between the intervention and control groups concerning the variable “Disease caused by mosquitoes” (P value = 0.001).
Table 4.
Intergroups comparison of scores at final (3-month) follow-up (n = 157)
|
Variables
|
Mean
|
SD
|
SE
|
P value
|
| Total score for disease caused by mosquitoes |
| Intervention |
5.68 |
0.470 |
0.037 |
0.001 |
| Control |
3.27 |
0.874 |
0.070 |
| Total score of knowledge |
|
|
|
|
| Intervention |
25.55 |
0.720 |
0.057 |
0.001 |
| Control |
12.81 |
3.193 |
0.255 |
| Total score of attitudes |
|
|
|
|
| Intervention |
21.06 |
2.480 |
0.198 |
0.001 |
| Control |
18.24 |
5.610 |
0.448 |
| Total score of practices |
|
|
|
|
| Intervention |
16.00 |
0.000 |
0.000 |
0.001 |
| Control |
4.37 |
1.882 |
0.150 |
Note. SD: Standard deviation; SE: Standard error.
Table 5 provides a summary of larval index measurements before and after the intervention, indicating a reduction in larvae in breeding sites. Initially, there were multiple baseline intervention instances at the locations (Larvae = 34, HI = 21.65) and baseline control group instances (Larvae = 31, HI = 19.74). However, after the intervention, there was a noticeable decrease in dengue cases in the intervention block compared to the control group (Larvae = 29, HI = 18.47).
Table 5.
Comparison of the number of dengue cases, larvae, and HI between intervention and control groups
|
Phase
|
Intervention Group (n=157)
|
Control Group (n=157)
|
χ2
|
P-value
|
|
Measuring Time
|
Found Larvae (n)
|
HI
|
Found Larvae (n)
|
HI
|
| Intervention baseline |
34 |
21.65 |
31 |
19.74 |
0.417 |
0.674 |
| Post-intervention data-1 |
7 |
04.45 |
- |
- |
2.675 |
0.007 |
| Post-intervention data-2 |
0 |
0 |
- |
- |
- |
- |
| Final follow-up |
0 |
0 |
0 |
29 |
5.656 |
0.001 |
Discussion
In the discussion, percentages and detailed results have been omitted, focusing on the interpretation of positive and negative outcomes, explanations, and references to relevant studies.
The intervention program aimed at enhancing dengue awareness and prevention within a poor urban community in Delhi, India, demonstrated significant positive outcomes. The study applied the HBM as the theoretical framework, focusing on knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, and preventive action.19
The intervention program aligned with the HBM theory, recognizing the importance of knowledge, perceived susceptibility, perceived severity, perceived benefits, and perceived barriers in shaping protective behaviors. The program was designed to bridge the gap between awareness and action, addressing the challenge of translating knowledge into practical measures to reduce mosquito populations.20
Various strategies were employed to enhance knowledge, including daily broadcasts, community-wide dengue campaigns, and group education sessions at the village hall. Additionally, a contest for a model house for dengue safety served as a cue to action, encouraging participants through positive community modeling. This multi-faceted approach aimed to foster a comprehensive understanding of dengue and promote preventive actions.21
Post-intervention, participants in the intervention group exhibited significantly higher scores across the six scales related to dengue hemorrhagic fever prevention compared to the control group. This outcome underscores the direct effectiveness of the intervention program. However, during the follow-up phase, some scores decreased, emphasizing the need for sustained community engagement to maintain the positive effects.22
The study highlighted the importance of community involvement in sustaining preventive actions. The decrease in scores during the follow-up phase suggests that continued efforts to enhance community engagement are crucial for long-term success. Encouraging behavioral change for dengue hemorrhagic fever prevention requires ongoing support, emphasizing the need for a sustained and collaborative approach within the community.23
The study observed a decrease in the HI for the intervention group post-intervention and during the follow-up. This decrease indicates the positive impact of the program on preventive actions, aligning with previous research linking knowledge of preventive measures to practical practices. To effectively reduce mosquito breeding sites, a community-wide shift in behaviors and sustained efforts are necessary.24-26
The study acknowledges potential reporting and social desirability bias, partly attributed to the researchers’ involvement. While structured survey techniques mitigate investigator influence, participant observation limitations were taken into consideration. Despite these drawbacks, the study emphasizes the value of health education initiatives in raising awareness and changing practices. Random sampling enhances the generalizability of findings.
Highlights
-
Tailored communication to address specific challenges faced by the urban poor
-
Engaged communities through workshops, awareness campaigns, and forums
-
Implemented innovative educational tools for effective information dissemination
-
Measurable improvements in dengue awareness levels and the adoption of preventive measures
-
Enhanced community collaboration with healthcare providers
-
Findings inform public health policies for urban areas
-
Recommendations for scaling similar interventions in resource-constrained settings
Conclusion
In general, the findings of this present study underscored the effectiveness of community-based interventions in enhancing knowledge and fostering the adoption of specific protective behaviors within impoverished urban areas. It is noteworthy that the focus of the intervention was not on measuring physical structures but on educating and engaging the local population.
While the study findings demonstrated that educational efforts can lead to positive behavioral changes, they also emphasized the insufficiency of education alone. Robust vector control measures and community-based environmental management strategies are essential complements to educational initiatives. These additional measures are crucial for inducing lasting behavior changes and, ultimately, eliminating diseases such as dengue.
Moreover, the study highlights the importance of providing healthcare workers with enhanced training in community engagement and communication. This aspect is imperative, especially in impoverished urban areas with a high prevalence of dengue fever. The HBM-based dengue fever prevention initiative employed in this study has proven successful in reducing the HI and increasing knowledge, perception of vulnerability, understanding of severity, overcoming barriers, and the adoption of preventive actions among residents in underdeveloped urban areas.
Therefore, the intervention program emerges as highly beneficial in effectively addressing the dengue issue within such an underprivileged metropolitan population. The findings suggest that a multifaceted approach, combining education, vector control, and community engagement, is crucial for sustained success in mitigating vector-borne diseases in similar contexts.
Acknowledgments
I express deep gratitude to Almighty God for His blessings throughout my journey. The success of this project is indebted to those who offered invaluable support, guidance, and feedback. I extend my sincere thanks to my supervisor, Associate Professor Dr. Rafdzah Binti Ahmad Zaki, for her patience and unwavering support during the field study. I also acknowledge the commitment of Associate Professor Dr. Nasrin Aghamohammadi and Professor Dr. Bratati Banerjee for their invaluable contributions. Special appreciation goes to the Department of Social and Preventive Medicine at the University of Malaya, my family for their love, and friends for their unwavering support. I am eternally grateful for the collaborative efforts that brought this project to fruition.
Authors’ Contribution
Conceptualization: Abhishek Lachyan, Rafdzah Ahmad Zaki.
Data curation: Abhishek Lachyan.
Formal analysis: Abhishek Lachyan, Rafdzah Ahmad Zaki.
Investigation: Abhishek Lachyan, Bratati Banerjee.
Methodology: Abhishek Lachyan, Rafdzah Ahmad Zaki, Bratati Banerjee, Nasrin Aghamohammadi.
Project administration: Abhishek Lachyan.
Resources: Abhishek Lachyan, Rafdzah Ahmad Zaki, Bratati Banerjee, Nasrin Aghamohammadi.
Software: Abhishek Lachyan.
Supervision: Bratati Banerjee, Rafdzah Ahmad Zaki, Nasrin Aghamohammadi.
Validation: Bratati Banerjee.
Visualization: Bratati Banerjee.
Writing–original draft: Abhishek Lachyan.
Writing–review & editing: Abhishek Lachyan, Rafdzah Ahmad Zaki, Bratati Banerjee, Nasrin Aghamohammadi.
Competing Interests
None declared.
Ethical Approval
The study received ethical approval from the University of Malaya Research Ethics Committee (UMREC) Malaysia (reference number UM.TNC 2/UMREC dated April 5, 2020) and the Institutional Ethics Committee (IEC) Maulana Azad Medical College and Associated Hospital, New Delhi, India (F.1/IEC/MAMC/79/07/2020/No.204 Dated on August 26, 2020).
Funding
There are no funding sources.
References
- Kusuma YS, Burman D, Kumari R, Lamkang AS, Babu BV. Impact of health education based intervention on community’s awareness of dengue and its prevention in Delhi, India. Glob Health Promot 2019; 26(1):50-9. doi: 10.1177/1757975916686912 [Crossref] [ Google Scholar]
- Hanklang S, Ratanasiripong P, Sivasan S. Effectiveness of the intervention program for dengue hemorrhagic fever prevention among rural communities in Thailand. J Health Res 2018; 32(5):352-63. doi: 10.1108/jhr-08-2018-042 [Crossref] [ Google Scholar]
- Abbas A, Abbas RZ, Khan JA, Iqbal Z, Hayat Bhatti MM, Sindhu ZU. Integrated strategies for the control and prevention of dengue vectors with particular reference to Aedes aegypti. Pak Vet J 2014; 34(1):1-10. [ Google Scholar]
- Anand T, Kumar R, Saini V, Meena G, Ingle G. Knowledge and use of personal protective measures against mosquito borne diseases in a resettlement colony of Delhi. Ann Med Health Sci Res 2014; 4(2):227-32. doi: 10.4103/2141-9248.129048 [Crossref] [ Google Scholar]
- Arunachalam N, Tyagi BK, Samuel M, Krishnamoorthi R, Manavalan R, Tewari SC. Community-based control of Aedes aegypti by adoption of eco-health methods in Chennai city, India. Pathog Glob Health 2012; 106(8):488-96. doi: 10.1179/2047773212y.0000000056 [Crossref] [ Google Scholar]
- Bhanu Vaishnavi G, Churi S, Narahari MG, Kurian J, Lalremruata B, Laldinpuii E. Study of impact of health education on knowledge, attitude and practice related to dengue fever. World J Pharm Pharm Sci 2015; 4(10):748-61. [ Google Scholar]
- Bhatnagar PK, Garg SK, Bano T, Jain S. Knowledge, attitude and practice regarding dengue and chikungunya in secondary school children in a city of North India. Eur J Pharm Med Res 2016; 3(11):423-8. [ Google Scholar]
- Boratne AV, Datta SS, Singh Z, Purty A, Jayanthi V, Senthilvel V. Attitude and practices regarding mosquito borne diseases and socio-demographic determinants for use of personal protection methods among adults in coastal Pondicherry. Indian J Med 2010; 1(2):91-6. [ Google Scholar]
- Ghosh A, Dar L. Dengue vaccines: challenges, development, current status and prospects. Indian J Med Microbiol 2015; 33(1):3-15. doi: 10.4103/0255-0857.148369 [Crossref] [ Google Scholar]
- Government of India. Ministry of Health and Family Welfare. Annual Report 2017-18. Available from: https://main.mohfw.gov.in/sites/default/files/00Introduction.pdf.
- Handel AS, Ayala EB, Borbor-Cordova MJ, Fessler AG, Finkelstein JL, Espinoza RXR. Knowledge, attitudes, and practices regarding dengue infection among public sector healthcare providers in Machala, Ecuador. Trop Dis Travel Med Vaccines 2016; 2:8. doi: 10.1186/s40794-016-0024-y [Crossref] [ Google Scholar]
- Heydari N, Larsen DA, Neira M, Beltrán Ayala E, Fernandez P, Adrian J. Household dengue prevention interventions, expenditures, and barriers to Aedes aegypti control in Machala, Ecuador. Int J Environ Res Public Health 2017; 14(2):196. doi: 10.3390/ijerph14020196 [Crossref] [ Google Scholar]
- Higuera-Mendieta DR, Cortés-Corrales S, Quintero J, González-Uribe C. KAP surveys and dengue control in Colombia: disentangling the effect of sociodemographic factors using multiple correspondence analysis. PLoS Negl Trop Dis 2016; 10(9):e0005016. doi: 10.1371/journal.pntd.0005016 [Crossref] [ Google Scholar]
- Ibrahim NK, Al-Bar A, Kordey M, Al-Fakeeh A. Knowledge, attitudes, and practices relating to dengue fever among females in Jeddah high schools. J Infect Public Health 2009; 2(1):30-40. doi: 10.1016/j.jiph.2009.01.004 [Crossref] [ Google Scholar]
- Kamel MN, Gnanakkan BD, Fauzi FZ, Hanafi MI, Selvarajah G, Jabar SA. The KAP study on dengue among community in Taman Salak Baiduri, Sepang, Selangor. Int J Sci Healthc Res 2017; 2(3):19-25. [ Google Scholar]
- Katyal R, Kumar K, Gill KS, Sharma RS. Impact of intervention measures on DF/DHF cases and Aedes aegypti indices in Delhi, India: an update, 2001. Dengue Bull 2003; 27:163-7. [ Google Scholar]
- Koenraadt CJ, Tuiten W, Sithiprasasna R, Kijchalao U, Jones JW, Scott TW. Dengue knowledge and practices and their impact on Aedes aegypti populations in Kamphaeng Phet, Thailand. Am J Trop Med Hyg 2006; 74(4):692-700. [ Google Scholar]
- Kumari A, Kant R, Sharma PK, Kumari M. Community knowledge, attitude, awareness and protective practices regarding malaria in Mewat and Rohtak districts of Haryana, India. Br J Med Med Res 2015; 8(12):1003-10. doi: 10.9734/bjmmr/2015/17311 [Crossref] [ Google Scholar]
- Malhotra V, Kaur P. The community knowledge, attitude and practices regarding dengue fever in field practice area of urban training health centre of Patiala. Int J Res Dev Health 2014; 2(1):19-26. [ Google Scholar]
- Mehta D, Solanki H, Patel P, Umat P, Chauhan R, Shukla S. A study on knowledge, attitude & practice regarding mosquito borne diseases in an urban area of Bhavnagar. Healthline J 2015; 6(2):29-32. [ Google Scholar]
- Siddiqui TR, Ghazal S, Bibi S, Ahmed W, Sajjad SF. Use of the health belief model for the assessment of public knowledge and household preventive practices in Karachi, Pakistan, a dengue-endemic city. PLoS Negl Trop Dis 2016; 10(11):e0005129. doi: 10.1371/journal.pntd.0005129 [Crossref] [ Google Scholar]
- Mohapatra S, Aslami AN. Knowledge, attitude and practice regarding dengue fever among general patients of a rural tertiary-care hospital in Sasaram, Bihar. Int J Community Med Public Health 2016; 3(2):586-91. [ Google Scholar]
- National Center for Vector-Borne Diseases Control (NCVBDC), Ministry of Health & Family Welfare. Dengue/DHF Situation in India. Available from: https://ncvbdc.mohfw.gov.in. Updated August 25, 2022. Accessed December 10, 2023.
- Vu SN, Nguyen TY, Tran VP, Truong UN, Le QM, Le VL. Elimination of dengue by community programs using Mesocyclops (Copepoda) against Aedes aegypti in central Vietnam. Am J Trop Med Hyg 2005; 72(1):67-73. [ Google Scholar]
- Park K. Park’s Textbook of Preventive and Social Medicine. 23rd ed. Jabalpur: Banarsidas Bhanot; 2015.
- Pramanik S, Punia M. Land use/land cover change and surface urban heat island intensity: source–sink landscape-based study in Delhi, India. Environ Dev Sustain 2020; 22(8):7331-56. doi: 10.1007/s10668-019-00515-0 [Crossref] [ Google Scholar]